

|
|
|



















Increasing efficacy of treatment in patients with steatohepatitis and concomitant chronic colitis
September 24, 2019
Звіт про довголіття: що нового в медицині та дослідженнях довголіття.
February 19, 2025Diagnosis and Treatment of Alcohol-Related Liver Diseases: 2019 Practice Guidance from the American Association for the Study of Liver Diseases

Authors: David W. Crabb, Gene Y. Im, Gyongyi Szabo, Jessica L Mellinger, Michael R. Lucey.
A. PURPOSE AND SCOPE OF THE GUIDANCE
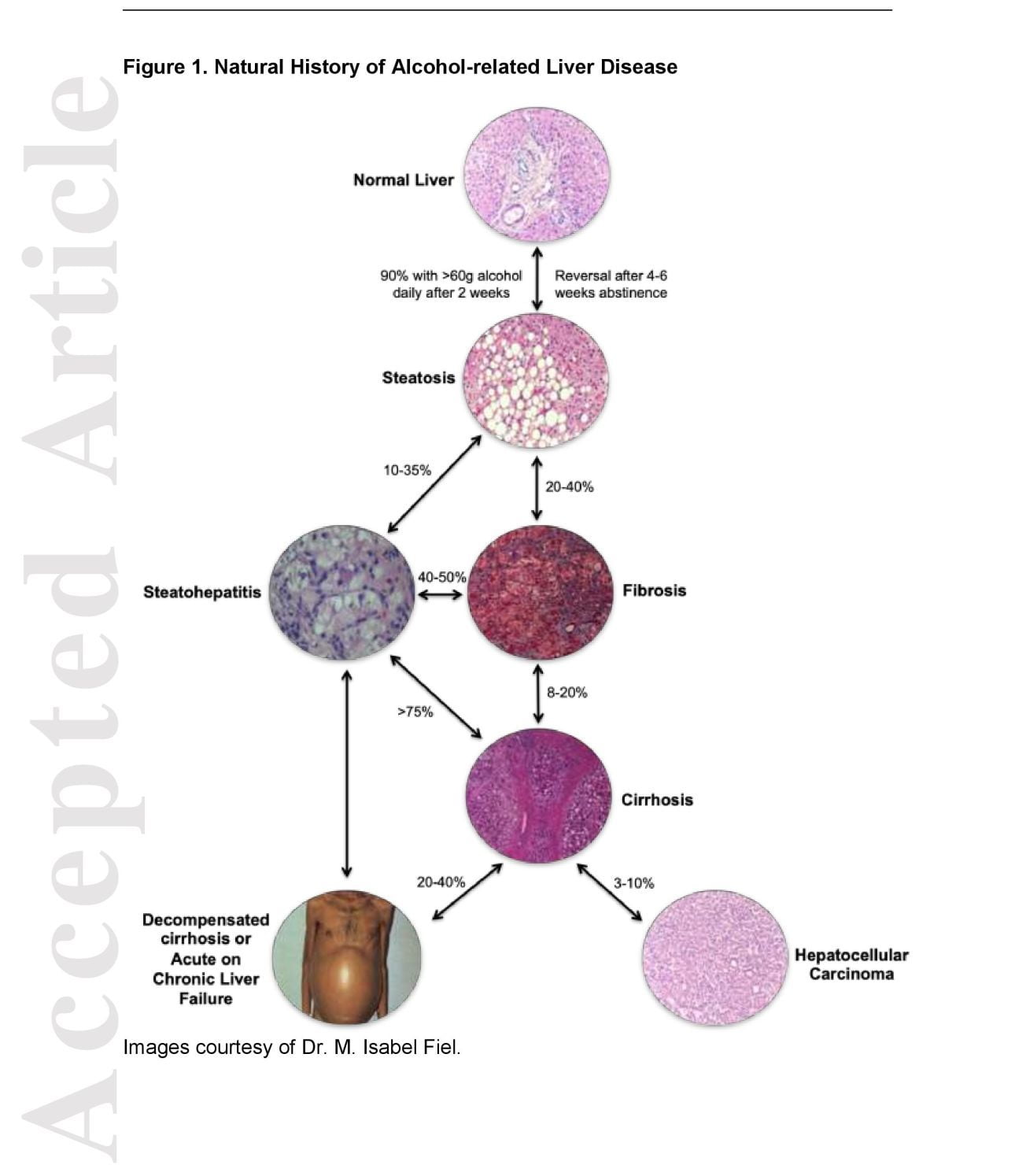
Alcoholic liver disease ( ALD) represents a spectrum of liver injury resulting from alcohol use, ranging from hepatic steatosis to more advanced forms including alcoholic hepatitis (AH), alcoholic cirrhosis (AC) , and acute alcoholic hepatitis presenting as acute on chronic liver failure (ACLF ). ALD is a major cause of liver disease worldwide, both on its own and as a co-factor in the progression of chronic viral hepatitis, nonalcoholic fatty liver disease (NAFLD ), iron overload and other liver diseases. ALD develops through several stages, beginning with hepatic steatosis, and, in some individuals, gradually progressing through alcoholic hepatitis (the histological correlate of which is alcoholic steatohepatitis ), culminating in cirrhosis (Figure 1). [1 , 2] Progression through these various stages is dependent upon continued heavy alcohol consumption and other risk factors, including female sex, genetic susceptibility, diet, and comorbid liver disease. ALD carries a significant stigma in society. It is increasingly recognized by providers that patients and their families seek to reduc e the stigma of alcoholic liver disease, and a change from the term “alcoholic” to “alcohol-related” will help; thus, alcohol-related liver disease, alcohol-related steatohepatitis , and alcohol-related cirrhosis are suggested, retaining the familiar abbreviations (ALD, ASH , and AC, respectively ) . Due to longstanding usage, the term alcoholic hepatitis (AH) will likely persist.
This 2019 ALD Guidance provides a data -supported approach to the prevalence, clinical spectrum, diagnosis and clinical management of ALD and alcohol use disorders (AUD). The guidance was developed by consensus of an expert panel and provides guidance statements based on formal review and analysis of published literature on the topics. The quality (level) of the evidence and the strength of each guidance statement are not formally rated. Updates to the 2010 Guidance include an em phasis on alcohol use disorder (AUD) definition, screening, and treatment; new alcohol biomarkers; additional genetic and environmental susceptibility factors; a consensus definition of AH, and review of recent studies of corticosteroids and guidance on the role of transplantation in the management of AH.
B. PREVALENCE AND BURDEN OF ALCOHOL-RELATED LIVER DISEASE
Alcohol-related liver disease includes a variety of clinical disorders: alcohol-related steatosis , alcoholic hepatitis (AH) of varying degrees of severity, alcohol-related cirrhosis (AC ), and AC complicated by hepatocellular carcinoma (HCC). ALD comprises a substantial portion of the overall cirrhosis burden both in the United States (US) and worldwide and is responsible for rising rates of liver-related mortality in the US, especially amongst younger patients. [3 , 4 , 5] In the US, mortality due to all ALD was estimated at 5.5 per 100,000 in 2012; the relative contribution of ALD to all cirrhosis mortality is predicted to increase as the proportion of deaths due to HCV cirrhosis declines. [3, 6] More recently, AC mortality was shown to have increased from 2008 -2016, particularly amongst patients ages 25 -34. [4] Cirrhotic and non -cirrhotic ALD prevalence has been estimated at ~2% in the general US population, while AC in the US Veteran’s population was estimated at 327 per 100,000 enrollees. [7 , 8] In privately insured US patients, AC has been estimated at approximately 100 per 100,000 enrollees and, overall, rates are projected to rise over time. [3, 9] Worldwide, AC deaths account for ~10% of all alcoho -attributable deaths and nearly half of deaths due to liver disease, resulting in the loss of 22.2 million disability -adjusted life years (DALYs) annually. [10 , 11] In the US, ALD competes with chronic hepatitis C (HCV ) as the leading indication for liver transplantation (LT). [12] Medical costs are high for AC, driven in part by the higher number of admissions for these patients. [9 ,13] In addition, deaths related to alcohol use are frequently under-estimated due to the stigma of alcohol use and lack of candor in reporting. [10 ,14] In women, AC prevalence may be increasing at a faster rate than in men, mirroring the rise in alcohol use in women in the US. [9]
The incidence of A H has been difficult to estimate as diagnostic accuracy of administrative coding is less reliable for AH. [15 , 16] The incidence of AH varies worldwide. In the US, admissions for AH were found to have increased to 0.83% of all admissions for 2010. [13] In Denmark, the incidence of AH for the period 1999 -2008 rose from 37 to 46 per million persons per year in men and 24 to 34 per million persons per year for women. [17] A similar study in Finland reported increased incidence rates for AH from 37 to 65 cases per million persons per year for men and from 13 to 27 cases per million persons per year for women. [18] In both of these cases, estimates were based on diagnostic coding, which may be less accurate and highlights the difficulty in estimating the burden of AH.
Accurate assessment of the full spectrum of ALD prevalence is challenging, particularly given the difficulty with identifying earlier, asymptomatic stages of ALD, such as alcohol-related steatosis or moderate AH, challenges that may be overcome with broader use of noninvasive steatosis and fibrosis assessment tools and increased awareness for the need to diagnose early stage disease. Many studies underestimate the true prevalence and burden by counting as ALD only those patients without additional liver diseases such as HCV, in spite of the fact that concomitant ALD rates are as high as 61% in some patients with other liver disease s , in particular nonalcoholic – steatohepatitis (NASH), HCV, and hemochromatosis. [14 ,19] These factors may result in as much as a two -fold underestimate for ALD-related mortality. [11]
C. DIAGNOSIS OF ALCOHOL USE DISORDERS
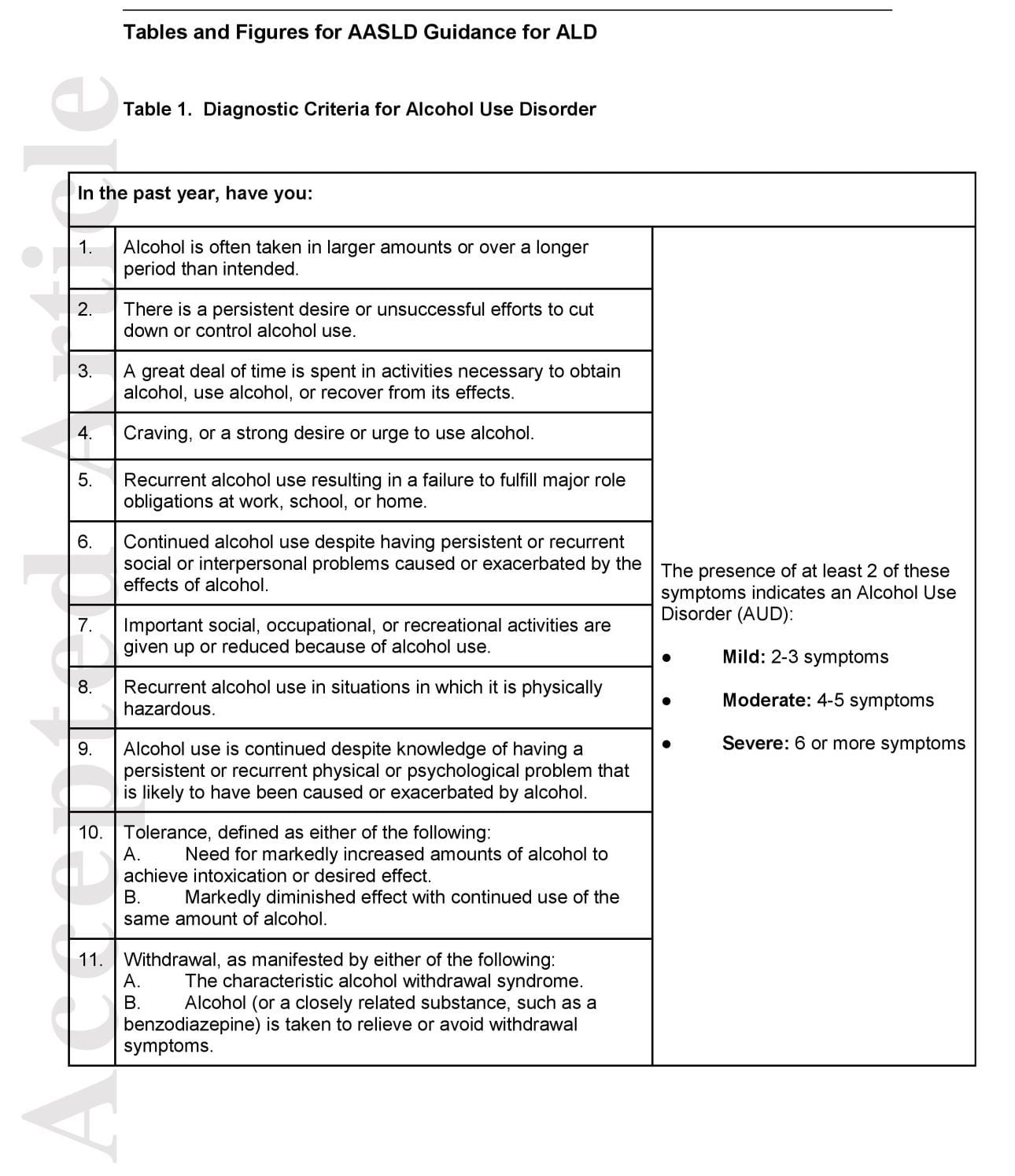
Since publication of the Diagnostic and Statistical Manual (5th Edition), the former categories of alcohol abuse and dependence have been replaced by the term alcohol use disorder (AUD), characterized as mild, moderate, or severe based on the accumulation of negative consequences and symptoms (Table 1). [20] Alcohol use is common in the US, with many people drinking moderate amounts without significant consequences. [21 , 22] However, more severe forms of AUD, defined by escalating alcohol consumption despite attempts to cut back, negative personal consequences, and the appearance of alcohol craving, are also on the rise. [21] Rates of AUD and high -risk drinking have risen dramatically, with the prevalence of AUD in 2 nationally representative surveys of US adults increasing by 50% between 2001 to 2013, with even greater increases reported amongst women, minorities , and those of lower socioeconomic status. [23] The type of alcohol consumed and the prevalence of binge drinking (≥5 drinks at a time occurring monthly or more often) changed over the same time period (2000 -2013) with substantial increases observed for consumption of distilled spirits (+11.5%), wine (+7.7%) and binge drinking. [23] Worldwide, alcohol consumption varies geographically, with the highest rates of reported per capita alcohol consumption occurring in northern and eastern European countries and Russia. [14]
a) SCREENING, BRIEF INTERVENTION AND REFERRAL TO TREATMENT
The public health approach to the problem of alcohol use is termed screening, brief intervention, and referral to treatment (SBIRT). This process begins with screening for and assessing the level of alcohol use. Discussion of alcohol use can be off -putting for patients, who may feel stigmatized or judged. [24] As such, a non -judgmental, open, and accepting interview style can help maintain therapeutic alliance, and limit under -reporting and denial of alcohol use disorders (AUD ). [25] The symptoms of AUD and ALD may not be readily apparent, particularly in early stages of ALD. The National Institute on Alcohol Abuse and Alcoholism (NIAAA) has published a brief guide for clinicians to help assess alcohol use, including more severe AUDs, provide brief intervention, pharmacotherapy, and refer more severe cases to treatment. [26] Of note, NIAAA guidelines for limits on drinking apply to general populations rather than patients with ALD; that is, there is no known safe level of alcohol consumption for patients with ALD. Similarly, the US Preventive Services Task Force (USPST F) has recently published its recommendations regarding ‘Unhealthy Alcohol Use in Adolescents and Adults: Screening and Behavioral Counseling Interventions’. The summary statement recommended ‘screening for unhealthy alcohol use in primary care settings in adults 18 years or older, including pregnant women, and providing persons engaged in risky or hazardous drinking with brief behavioral counseling interventions to reduce unhealthy alcohol use. [27]
Efforts to uncover harmful alcohol use are aided by the use of structured, validated screening tools. The NIAAA recommends a one -question initial screen: “How many times in the past year have you had 5 or more drinks in a day (for men) or 4 or more drinks in a day (for women)?” This is the NIAAA definition of binge drinking (5 drinks in men; 4 in women over 2 hours). If the patient reports even a single episode, performing the Alcohol Use Disorders Inventory Test (AUDIT) is recommended. The AUDIT is widely used and is also recommended by the United States Preventive Services Task Force (USPSTF). Its original form included 10 questions on consumption (Q1 -3), dependence symptoms (Q4 -6) , and any alcohol-related problems (Q7 -10) with a score >8 being predictive of harmful or hazardous alcohol use and scores >20 suggestive of alcohol dependence (now termed moderate/severe AUD). [22 , 28] Questions 1-3 are often used alone (the “AUDIT – C”) as a more efficient means of screening for problem alcohol use, but this shorter form does not provide information on more severe alcohol use problems. [29] The AUDIT – C is brief, convenient, and performs better than the CAGE and other questionnaires in identifying alcohol misuse. [30] AUDIT -C scores ≥4-5 may indicate harmful alcohol use. These screening tests do not provide a diagnosis of AUD, but rather point to the need for a formal assessment. The NIAAA Clinicians’ Guide outlines brief intervention and referral to treatment for the general public; space limitations prevent a more thorough discussion of brief interventions. [31]
Screening in general medicine and specialty clinics has been shown to help identify ALD patients early, and by coupling this to a discussion of the implications for liver disease, may be motivational for alcohol reduction. [32] Mandatory alcohol use screening in inpatient s and the emergency department effectively identifies heavy users, assists ALD diagnosis, and improves connection to treatment of AUD. [33] Importantly, use of screening tools such as AUDIT has been shown to improve detection as well as the ability to predict long -term clinical outcomes, including hospitalization for alcohol-related diagnoses. [34, 35]
b) BIOMARKERS OF ALCOHOL USE
Biomarkers of alcohol use refer to moieties in urine, blood, or hair which identify metabolites or surrogates of alcohol use, and provid e an estimated timeframe of recent drinking. The American Society of Addiction Medicine (ASAM) and American Psychiatric Association (APA) suggest the use of alcohol biomarkers as an aid to diagnosis, to support recovery and as catalysts for discussion with the patient, rather than as tools to “catch” or punish patients. [36, 37] Principles of use include discussing biomarker use with patients prior to testing in order to maintain therapeutic alliance and improve alcohol use disclosure. Each of the alcohol biomarkers described below has limitations. They should not be used on their own to confirm or refute alcohol use , but should be combined with other lab testing (including other alcohol biomarkers), physical exam, and the clinical interview.
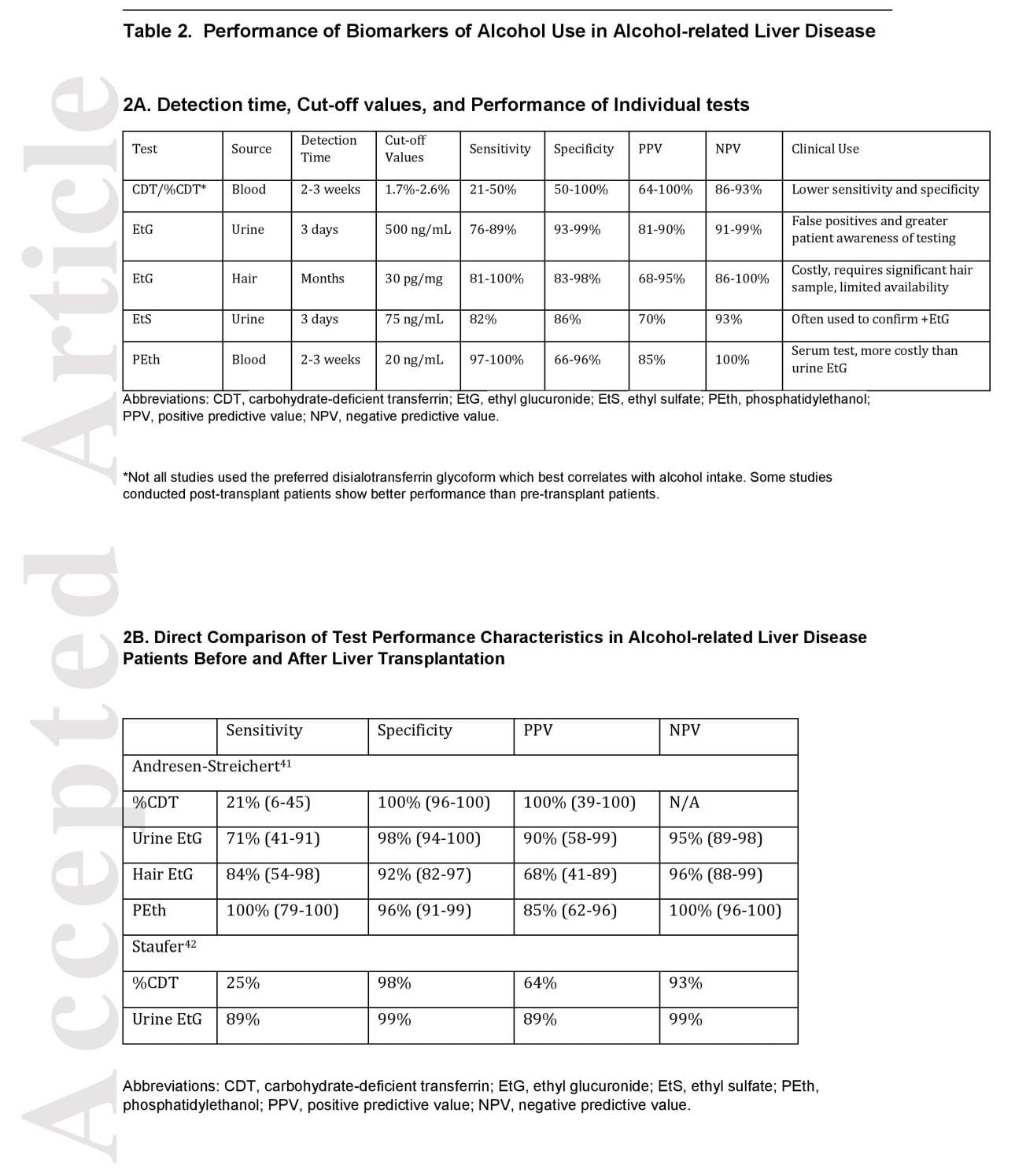
Liver-related enzymes, bilirubin, or gamma-glutamyl transferase (GGT) or evidence of macrocytic anemia may suggest alcohol use but, on their own, are inadequate to establish alcohol use in ALD. [38, 39] GGT is an enzyme found in the cell membranes of several body tissues, including liver and spleen. While it is frequently elevated in heavy drinking and has greater sensitivity than AST, it is not specific for alcohol use. [40] Carbohydrate-deficient transferrin (CDT) is generated as a result of alcohol inhibition of transferrin glycosylation. Typically reported as the % CDT/ total transferrin, to account for differences in total transferrin levels, CDT has a half-life of 2 -3 weeks. [41] The utility of CDT is limited by its low sensitivity of 25-50% in several studies and by false positive results arising in patients with severe liver disease in the absence of alcohol use. [42, 43, 44, 45, 46] However, post -transplant use of %CDT appears to be more accurate, likely due to improved liver function. [47, 48]
A small (~0.1%) amount of alcohol is metabolized by UDP -glucuronosyltransferase and -sulfotransferase, producing ethyl glucuronide (EtG) and ethyl sulfate (EtS). [49] Both are excreted in the urine, but are also found in blood and hair. Although false positives and false negatives have been reported, sensitivity and specificity of urinary EtG for detection of alcohol use were 89% and 99% respectively among ALD patients before and after liver transplantation (LT). [43] Other studies in patients with mixed etiology of liver disease, including cirrhosis, found sensitivities of 76% and 82% for drinking within 3 -days of the test for EtG and EtS, respectively, with higher specificities of 93% and 86%, respectively.50 Urinary EtG and EtS detection times can also be prolonged in renal failure resulting in a longer window of positive results after alcohol ingestion in patients with kidney disease.
Phosphatidylethanol (PEth) is a phospholipid formed by the reaction of phosphatidylcholine with ethanol catalyzed by phospholipase D in the erythrocyte cell membrane. [51] PEth has a half -life of approximately 10-14 days, although this can be longer with more chronic, repeated heavy alcohol consumption and does not appear to be influenced by age, body mass index (BMI), sex, kidney or liver disease. [51, 52, 53, 54, 55, 56, 57] Women may have higher PEth levels for a given amount of alcohol consumption compared to men. [58] Although there are inter -individual variations in PEth metabolism, PEth has been validated in a study of chronic liver disease patients who had not undergone LT at a cut -off of 80 ng/mL for 4 drinks per day or more with a sensitivity of 91% (95% confidence interval (CI), 82 -100%) and specificity of 77% (95% CI, 70 -83%). [59] Another study of PEth use in ALD patients before and after LT revealed a sensitivity of 100% (CI, 79 -100%) and specificity of 96% (CI, 91 -99%) for a cut -off of >20 ng/mL. [42] The performance of the current best biomarkers for alcohol use are shown in Table 2.
Guidance Statements
- All patients receiving care in primary care and gastroenterology/hepatology outpatient clinics, emergency departments, and inpatient admissions should be routinely screened for alcohol use using validated questionnaires.
- Brief intervention, pharmacotherapy, and referral to treatment should be offered to patients engaged in hazardous drinking (AUDIT – C ≥4, AUDIT >8, binge drinkers)
- Alcohol biomarkers can be used to aid in diagnosis and support recovery. Urine and hair ethyl glucuronide, urine ethyl sulfate, and PEth are not affected by liver disease, and therefore preferable.
D. TREATMENT OF ALCOHOL USE DISORDER S
Since abstinence is the single most important factor in improving survival from ALD, multidisciplinary management with addiction specialists and referral to treatment for AUD, particularly in patients with moderate to severe AUDs or clinically evident ALD, is mandatory. We present a review of different types of treatment, with a focus on treatments that have been studied in patients with ALD. Many patients, however, will be reluctant to see a professional mental health provider. For patients ambivalent about alcohol cessation, motivational interviewing has been shown to help patients change behaviors, including alcohol use. [60] A new online resource developed by NIAAA is now available to help people and their families recognize AUD and find high quality care t hrough an easily accessible and user -friendly web -based system, the NIAAA Alcohol Treatment Navigator. [61]
a) PSYCHOSOCIAL AND BEHAVIORAL APPROACHES TO ALCOHOL USE TREATMENT IN ALD PATIENTS
There are a wide variety of alcohol use treatments available to patients, though relatively few have been studied in ALD patients. Major categories of treatment include inpatient alcohol rehabilitation, group therapies, individual therap y, family/couples counseling, and mutual aid societies (such Alcoholics Anonymous (AA) ). Within counseling sessions, various modalities of treatment are available which target different mechanisms of behavior change. These include cognitive-behavior therapy (CBT), motivational interviewing (MI), motivational enhancement therapy (MET), contingency management, 12-step facilitation, network therapy, and couples/family counselling. [25]
Psychosocial treatment has been studied in a limited fashion in ALD. A recent systematic review of treatment trials in ALD found that integrating AUD treatment providers alongside medical providers in clinic produced better abstinence rates than usual care, which typically means a referral to a treatment provider outside the liver center. [62]
Types of AUD treatment evaluated in both randomized and observational trials include CBT, MET, psycho -education, and motivational interviewing, with modalities combined in varying ways in each trial. Five randomized controlled trials were reported, 3 of which enrolled AC patients exclusively and only one of which showed statistically significant benefit with an integrated intervention combining alcohol use treatment with medical care. [63, 64, 65] Other observational studies evaluated psychosocial interventions for HCV patients with AUD and showed modest improvement in abstinence with integrated care again producing improved outcomes. [66, 67, 68, 69] However there are few data to show that one treatment modality is consistently superior to another across all categories of populations. [70] Based on these findings, integrated, multidisciplinary care remains the best option for management of advanced ALD and AUD, although may not be practical in all resource settings. [71]
b) RELAPSE PREVENTION MEDICATIONS
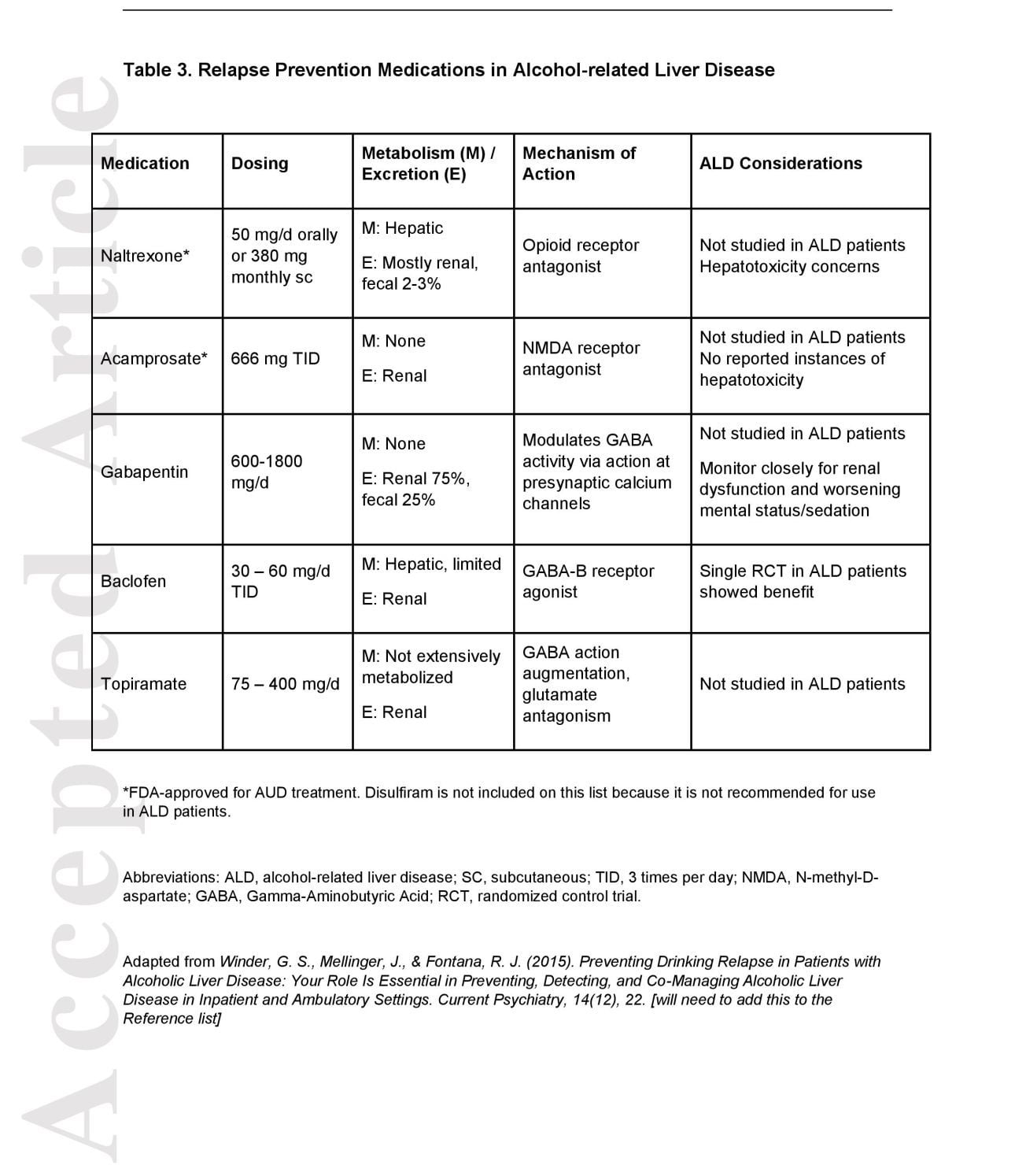
Pharmacotherapy for AUDs includes both FDA and non-FDA approved medications shown in Table 3. There are three FDA-approved medications: disulfiram, naltrexone, and acamprosate. The number needed to treat to prevent return to any drinking is estimated to be approximately 12 for acamprosate and 20 for naltrexone. Disulfiram and naltrexone undergo hepatic metabolism and can cause liver damage, while acamprosate has no hepatic metabolism. Of note, none of these medications have been studied in patient s with AH and AC. In addition, there are several medications with some benefit in relapse prevention which have not been FDA -approved for AUD treatment. These agents include gabapentin, baclofen, topiramate, ondansetron, and varenicline. [72, 73, 74, 75] Baclofen, a GABA -B receptor agonist, is the only AUD pharmacotherapy that has been tested in a randomized controlled fashion in AC patients with AUD as well as in two small , uncontrolled observational studies. [72, 76, 77] In a randomized trial comprising both compensated and decompensated AC patients, a 12 -week course of baclofen (10 mg three times daily) resulted in improved rates of total alcohol abstinence and decreased relapse compared to the control during one year of observation while exhibiting an acceptable safety profile. [72, 78] Notably, patients with HE were excluded from this trial since baclofen may impair mentation, a side effect which may be exacerbated in more advanced liver disease. Based on limited data, and in the absence of a RCT demonstrating efficacy, acamprosate does not appear to be toxic to the liver and is probably safe.
Guidance Statements
- Referral to AUD treatment professionals is recommended for patients with advanced ALD and/o r AUD in order to ensure access to the full range of AUD treatment options.
- Multidisciplinary, integrated management of ALD and AUD is recommended and improves rates of alcohol abstinence amongst ALD patients.
- Based on limited data, the use of acamprosate or baclofen can be considered for the treatment of AUD in patients with ALD.
E. PATHOPHYSIOLOGY AND RISK FACTORS FOR ALCOHOL-RELATED LIVER DISEASE
Given the widespread levels of heavy alcohol use worldwide, it is clear that a minority of heavy drinkers develop significant liver disease. The injurious effect of alcohol on the liver is not linearly dose -dependent, but there is a threshold beyond which the risk for serious liver disease increases with increasing levels of consumption. [79] According to the “Dietary Guidelines for Americans 2015 -2020,” U.S. Department o f Health and Human Services and U.S. Department of Agriculture, the upper limit of safe drinking appears to be one standard drink per day for women and 2 standard drinks for men. [80] Furthermore, the NIAAA defines binge drinking as a pattern of drinking that brings blood alcohol concentration (BAC) levels to 0.08 g/dL, and which typically occurs after 4 drinks for women and 5 drinks for men —in about 2 hours. [81] The Substance Abuse and Mental Health Services Administration (SAMHSA), which conducts the annual National Survey on Drug Use and Health (NSDUH), uses an almost identical definition while adding ‘on at least 1 day in the past month’. By NIAAA definition, a standard drink contains 14 g alcohol (equivalent to 12 oz beer (5% alcohol), 8 -9 oz malt liquor, 5 oz table wine, or 1.5 oz distilled spirits). [82] A simplification would be to adopt the European standard that one standard measure of any form of alcohol is constituted by 10 g. The upper threshold of safe consumption continues to be reviewed, with a recent analysis suggesting alcohol use should be limited to one drink per day for men and women, or even that any drinking may have adverse health consequences. [83, 84]
The pathophysiology of ALD is complex. Heavy use results in accumulation of fat through effects on redox state of the liver and on a number of transcription factors which regulate pathways involved in fatty acid synthesis (increased) and oxidation (decreased). In some individuals, changes in gut permeability lead to increased portal vein endotoxin, activation of the innate immune response, and liver cell inflammation, injury, apoptosis and necrosis, and fibrosis via cytokine and oxidative stress cascades. These cascades involve interactions between the resident macrophages (Kupffer cells), myofibroblasts, endothelial cells, and hepatocytes. [85] Interruption of these pathways has resulted in improvement in liver injury, and t hese results help explain current therapy with anti -inflammatory and anti -oxidant agents. There are ongoing trials examining anti -cytokine and gut -directed therapies.
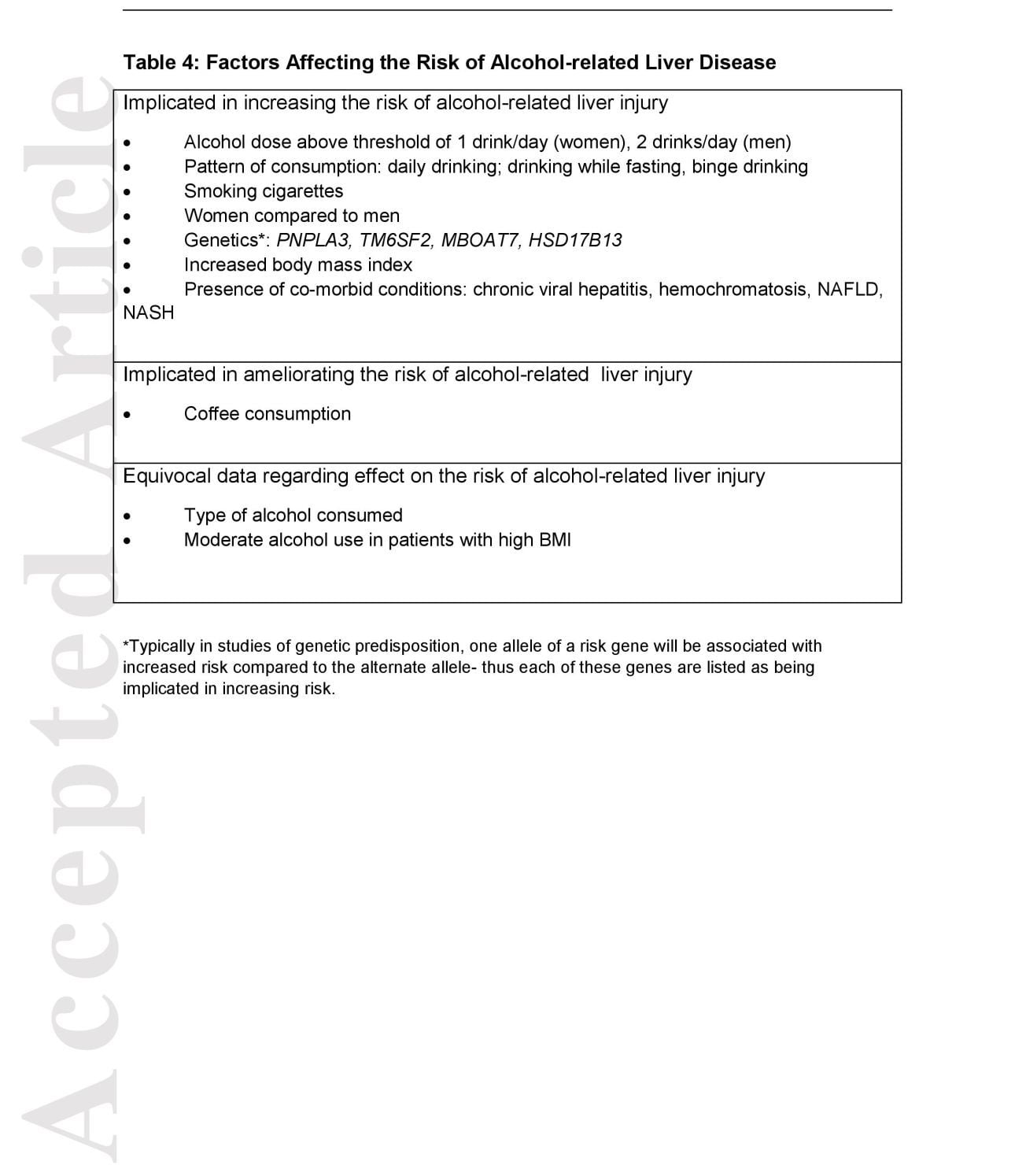
Table 4 lists factors that influence the risk of alcohol -related liver injury. [86, 87, 88, 89, 90, 91] Women have a greater risk of liver injury compared to men for any level of drinking. [88] Wine consumption was less likely to be associated with cirrhosis than other beverages. [89] Daily drinking conferred greater risk of ALD and smoking independently increases the risk for cirrhosis. [90, 91] A meta -analysis of studies of alcohol consumption and cirrhosis risk confirmed increased risk for women. [78] There is evidence that binge drinking increases the risk of ALD. [92] Coffee consumption protects against cirrhosis of many causes including ALD as well as AH. [93, 94, 95, 96, 97]
Studies of mono – vs dizygotic twins suggest a heritability of about 50% for AUD, and subsequent genome -wide studies show this to be a complex polygenic disorder. [98, 99] Polymorphisms in the alcohol metabolizing genes alcohol dehydrogenase 2 (ADH2) and aldehyde dehydrogenase 2 (ALDH2 )have been strongly linked to risk of AUDs, but not with risk of liver disease. [100] Polymorphisms in the gene for the alcohol oxidizing enzyme, cytochrome P450 Family 2 Subfamily E Member 1 (CYP2E1 ) confer a minor risk for ALD. [101] Studies of racial and ethnic predisposition have shown that Hispanics are at substantially increased risk of developing alcohol – and non -alcohol -related steatosis, steatohepatitis and cirrhosis, and of developing AH compared with non -Hispanic Whites and African – Americans. [102, 103]
Genetic variants have been associated with differential risk of ALD. Patatin-like phospholipase domain -containing protein 3 (PNPLA3) polymorphism has been associated with risk of AC and AH, as have polymorphisms in the transmembrane 6 superfamily member 2 (TM6SF2), and membrane bound O-acyltransferase domain-containing 7 (MBOAT7) genes. [104, 105, 106, 107] PNPLA3 and TM6SF2 polymorphisms are also associated with increased risk of hepatocellular carcinoma in ALD. [108, 109] Most recently, Abul -Husn et al. have described a polymorphism related to a hepatic lipid droplet protein hydroxysteroid 17 – beta dehydrogenase 13, HSD17B13, the presence of which confers protection against the progression from steatosis to steatohepatitis in alcohol- and non-alcohol-related chronic liver disease. [110]
Co-existent heavy alcohol use by patients with certain other liver diseases promotes the development of advanced fibrosis and cirrhosis. The most common are NAFLD, HCV, and hemochromatosis. Even moderate alcohol use in NAFLD may worsen fibrosis and risk of HCC. [111] Conversely, the different elements of the metabolic syndrome were found to be important risk factors for alcohol-related liver injury. [112] The interaction between alcohol use and progression of HCV disease is well-established: a recent French study showed that the patients with concomitant AUDs had greatly increased risk of liver complications, need for transplantation, and liver -related death. [113] Alcohol use (above 60 g/day) was also associated with a markedly increased risk of cirrhosis in patients with hemochromatosis. [114]
Guidance Statements
- Patients without liver disease should be educated about safe levels of alcohol consumption for men (no more than 2 standard drinks per 24 hours) and women (no more than 1 standard drink per 24 hours).
- Patients with ALD or other liver diseases, in particular NAFLD, NASH, viral hepatitis, and hemochromatosis, should be counseled that there is no safe level of drinking, and that they should abstain.
F. DIAGNOSIS AND TREATMENT OF ALCOHOL-RELATED LIVER DISEASES
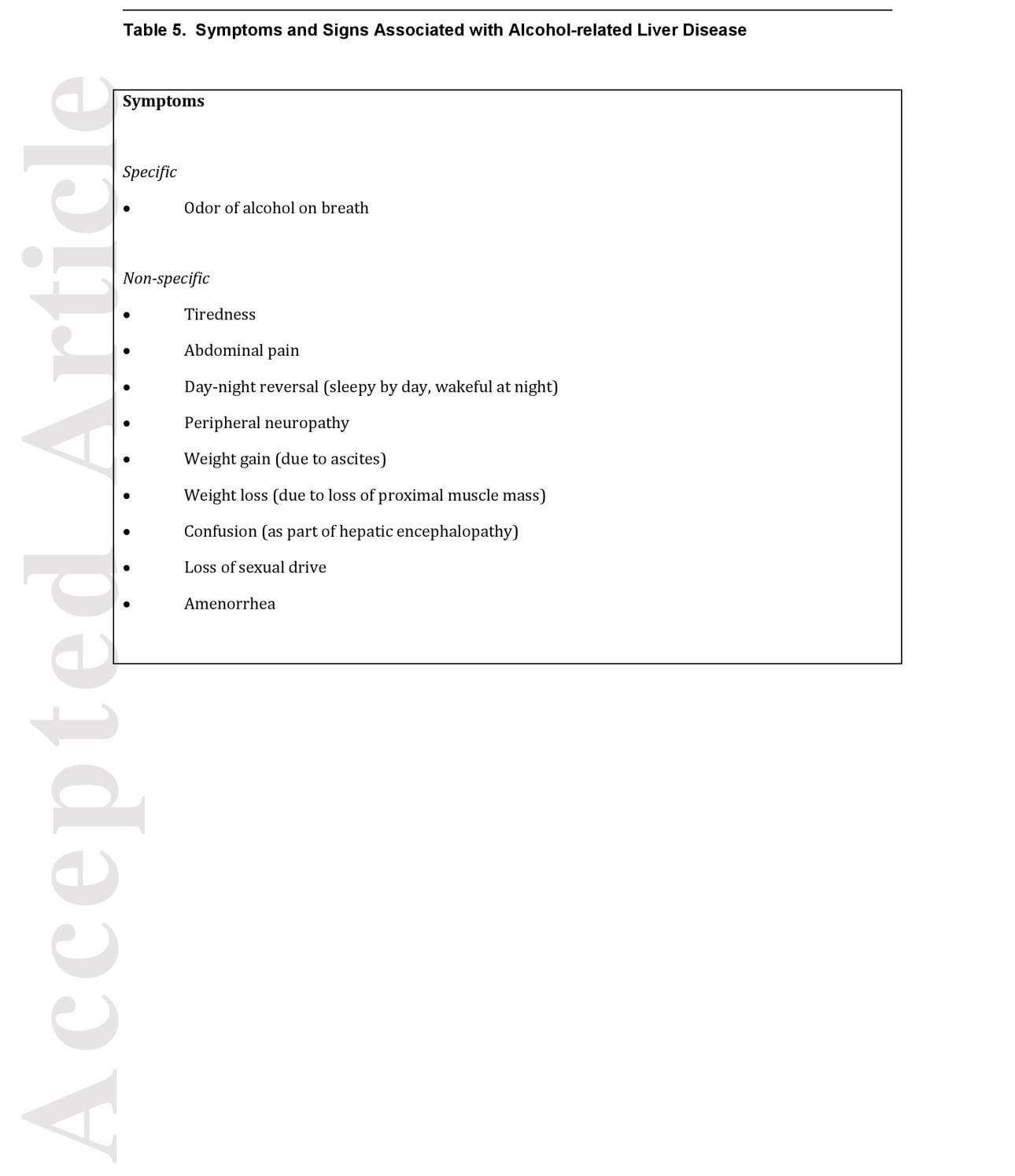
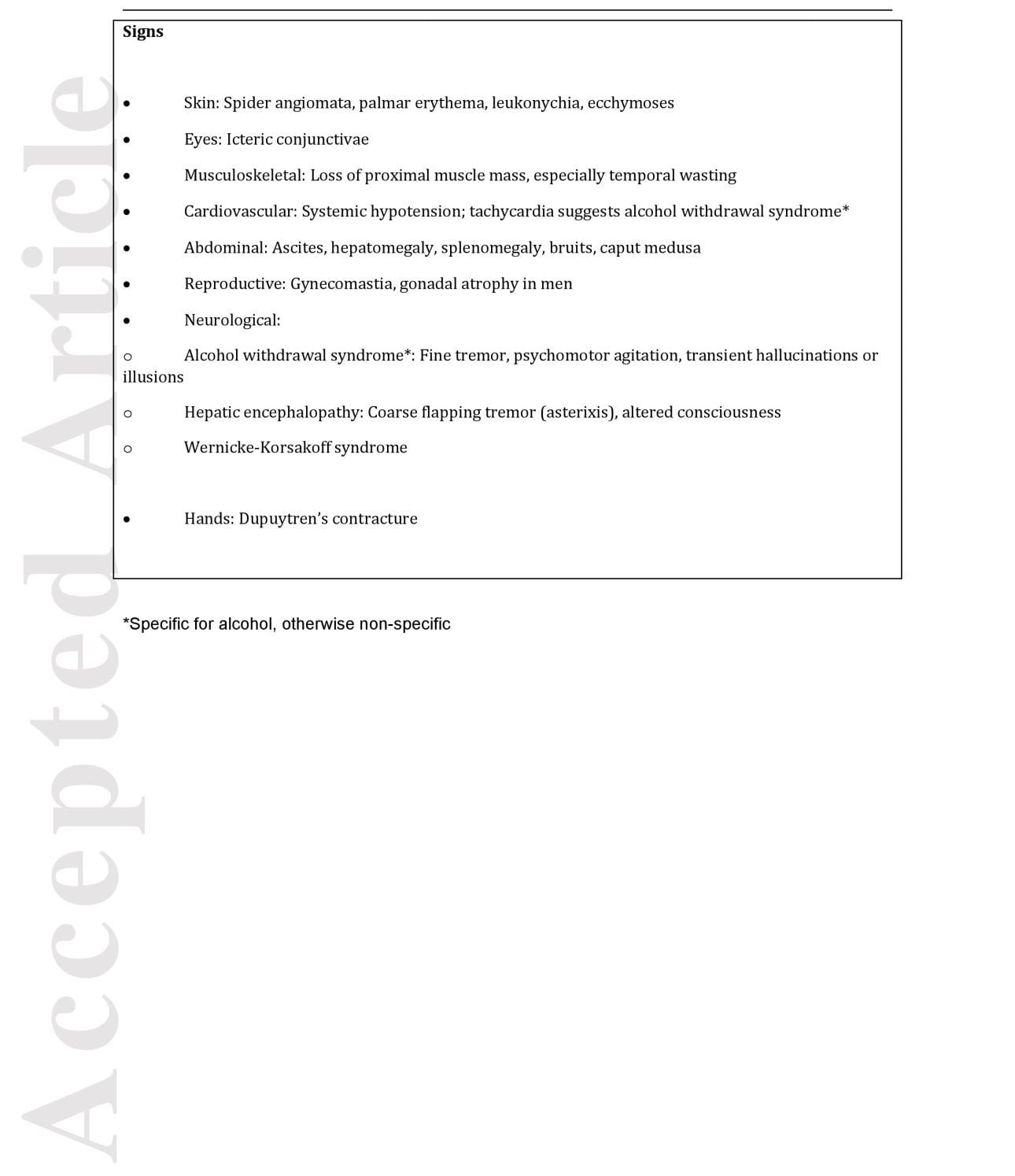
There is no unique presentation of ALD which can be distinguished with confidence from other forms of liver disease. Alcohol use is often not disclosed by the affected patient, while liver injury, whether due to alcohol or other causes, often proceeds silently. Although not all patients with ALD meet criteria for AUD, failure to recognize AUD remains a significant clinical problem. [115] Providers need to have a high index of suspicion for AUD in patients presenting with non -specific symptoms and signs shown in Table 5. [116]
a) ALCOHOL -RELATED STEATOSIS
Patients with alcohol -related steatosis are usually asymptomatic. A palpably enlarged liver may be found in the absence of jaundice or stigmata of advanced liver disease. Among the common liver enzymes, elevations of AST and GGT are the best indicators of recent excessive alcohol consumption. [117, 118] Hepatic steatosis is readily identified on sonography, CT and MR imaging of the liver. [119] MRI is more accurate for quantifying fat than other radiologic techniques, with the added advantage that MRI can assess fat over the entire volume of the liver. [120] Liver biopsy is rarely needed for the diagnosis of alcohol-related steatosis. Treatment consists of avoidance of alcohol, with attention to the common association with NAFLD; thus lifestyle measures that address obesity, physical activity, and alcohol use are often needed. Alcohol -related steatosis is reversible with cessation of alcohol use.
b) ALCOHOL-RELATED CIRRHOSIS
Cirrhosis is often diagnosed at the time of decompensation, or may be uncovered in the course of evaluating abnormal physical findings or laboratory tests. Signs and symptoms are listed in Table 5. Abdominal imaging may reveal hepatic nodularity or signs of portal hypertension, and transient elastography may provide evidence of increased liver stiffness. AC cannot be differentiated from other causes of cirrhosis except through careful evaluation of drinking history and exclusion of other causes of liver disease. The prognosis of AC is assessed just as other forms of cirrhosis, namely using the Child-Turcotte-Pugh (CTP) and the Model for End-stage Liver Disease (MELD or MELD-Na ) score. The outcome of AC is crucially influenced by the patient’s ability to abstain, both to slow the progression of fibrosis and its consequences, and in anticipation of evaluation for liver transplantation. It is important to realize that decompensation of a cirrhotic patient may reflect the onset of AH, since the majority of patients with AH have already developed AC ; thus an opportunity for treatment may be lost.
c) ALCOHOLIC HEPATITIS
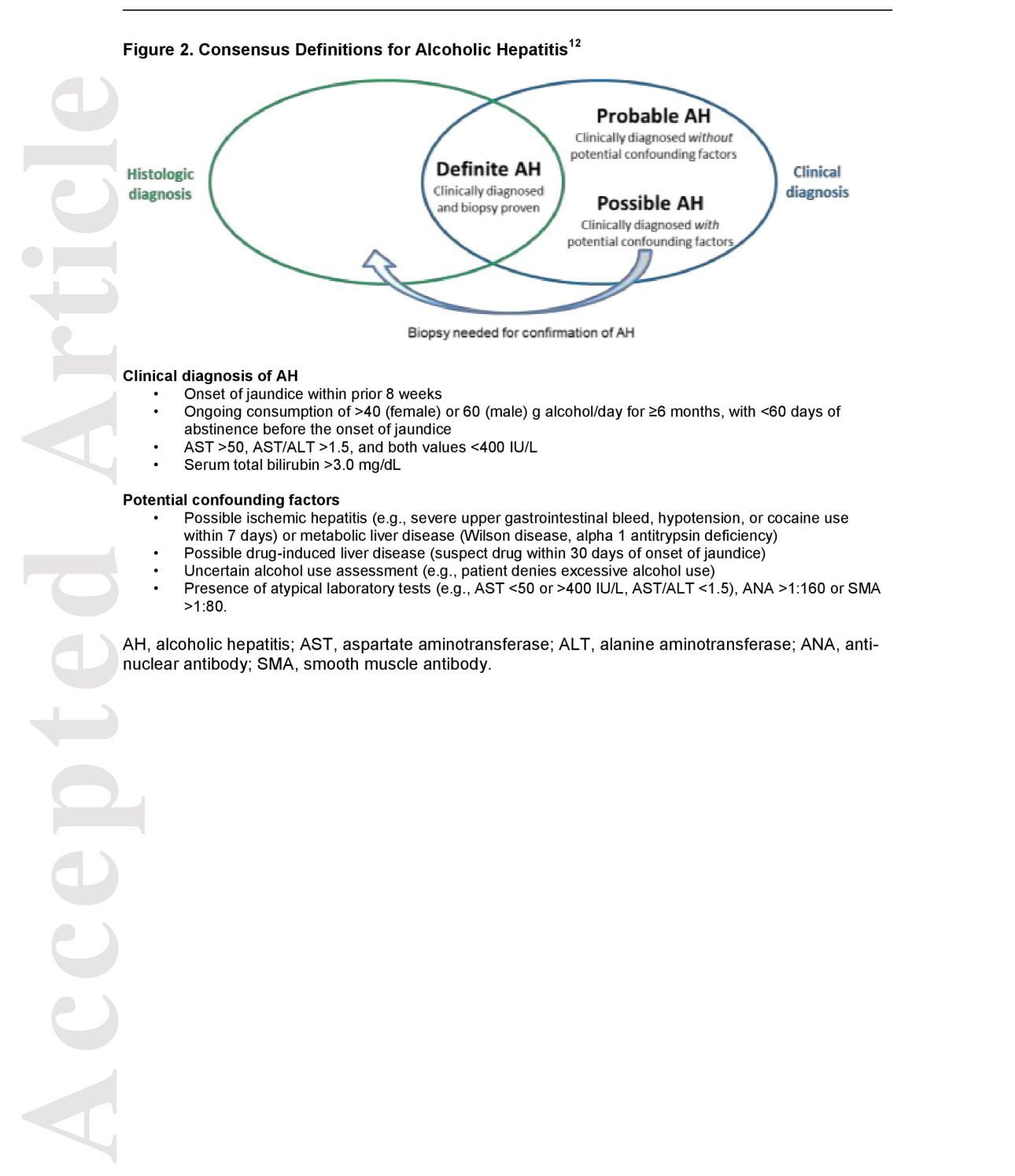
There is a broad spectrum of clinical presentation of patients with AH who may exhibit few signs or symptoms, or present with liver failure. AH per se is a clinical syndrome (criteria are described below and in Figure 2) with a distinct histopathological correlate, called alcohol -related steatohepatitis (ASH). The histological features of AH may be present in patients with no symptoms and mild laboratory abnormalities. Its histological features comprise neutrophilic lobular inflammation, degenerative changes in hepatocytes (ballooning and Mallory -Denk inclusions), steatosis, and pericellular fibrosis. [121] However, these features are variable in individual cases, and are often co -existent with frank cirrhosis. In addition, liver biopsy cannot distinguish between ASH and NASH. The role of liver biopsy is therefore to resolve diagnostic dilemmas and to establish consistency regarding AH in patients recruited to clinical trials. [122] However, since uncertainty persists in a fair number of patients, a consensus statement reg arding the clinical diagnosis AH, and when biopsy confirmation of ASH was most valuable, was published in 201 6. [123] The statement was intended to improve consistency in diagnosis of AH across research studies and clinical trial s, and to guide clinical decision making about the use of potentially toxic medications such as corticosteroids (Figure 2). It categorizes patients with putative AH into three groups: those with biopsy -proven AH, those with probable AH, and those with possible AH who would require biopsy confirmation of histological features of ASH.
Non-invasive tests for AH are sorely needed. A study of a panel of serum biomarkers of liver injury and inflammation in patients with AH demonstrated that circulating fragments of cytokeratin-8 (CK-18) and the main constituent of Mallory -Denk bodies, termed M65 and M30, both had an area under the receiver operating characteristics curve of 0.84 to estimate the presence of AH. [124] These data suggest that we may have biomarkers that have diagnostic significance for AH soon. Also, there may be characteristic “breathprints” in AH. [125] Transient elastography (TE) and serum liver fibrosis markers like Enhanced Liver Fibrosis test (ELF) and FibroTest may have a role in assessing fibrosis in compensated ALD, and in following improvement of inflammation with recovery. [126, 127, 128] At present, none of these have been adequately validated for routine clinical use in the diagnosis of AH.
Guidance Statements
- The diagnosis of AH (definite, probable, possible) should be made using the published consensus criteria (Figure 2).
d) ASSESSING PROGNOSIS IN ALCOHOLIC HEPATITIS
d) 1. Lab -based Prognostic Scores
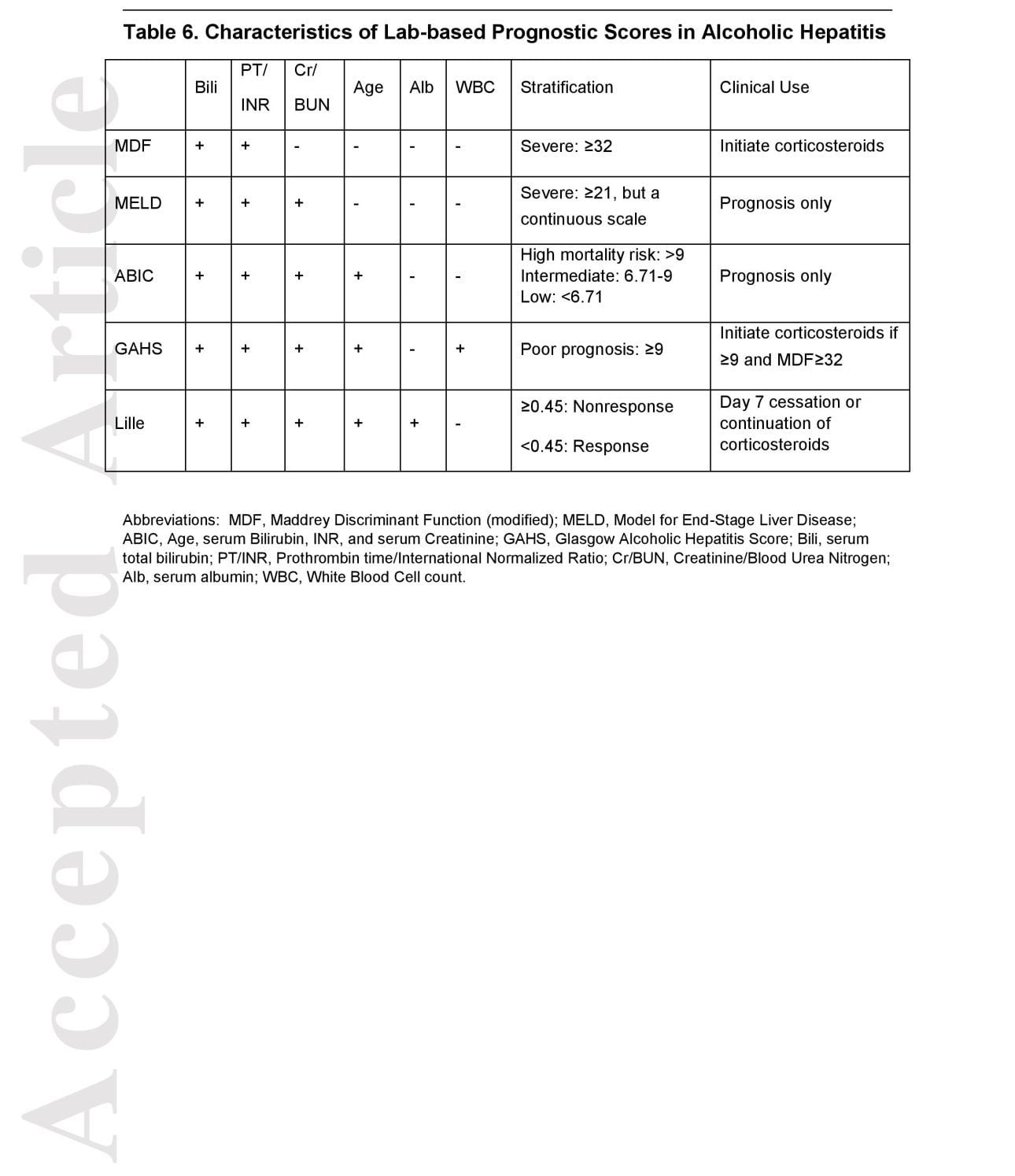
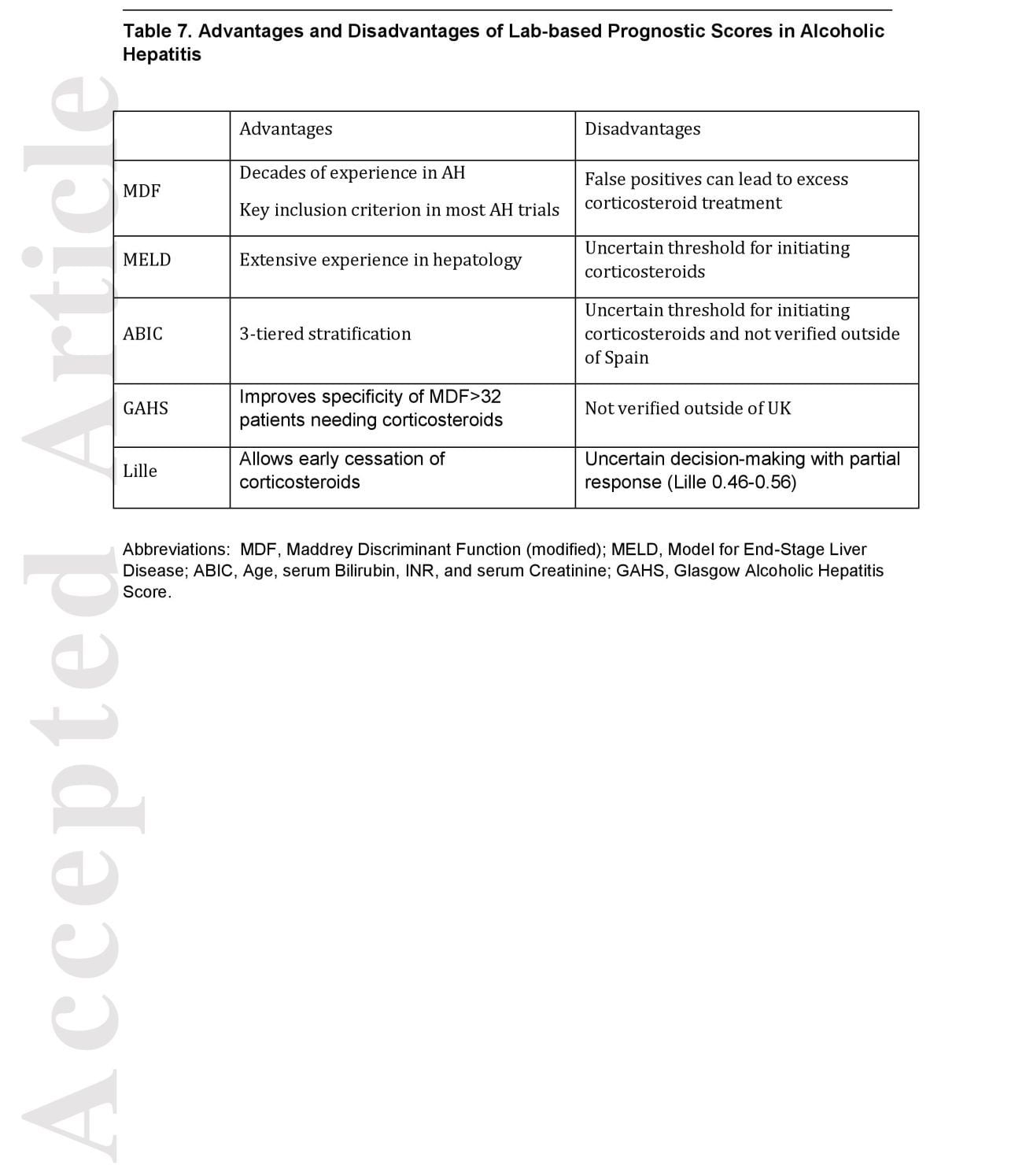
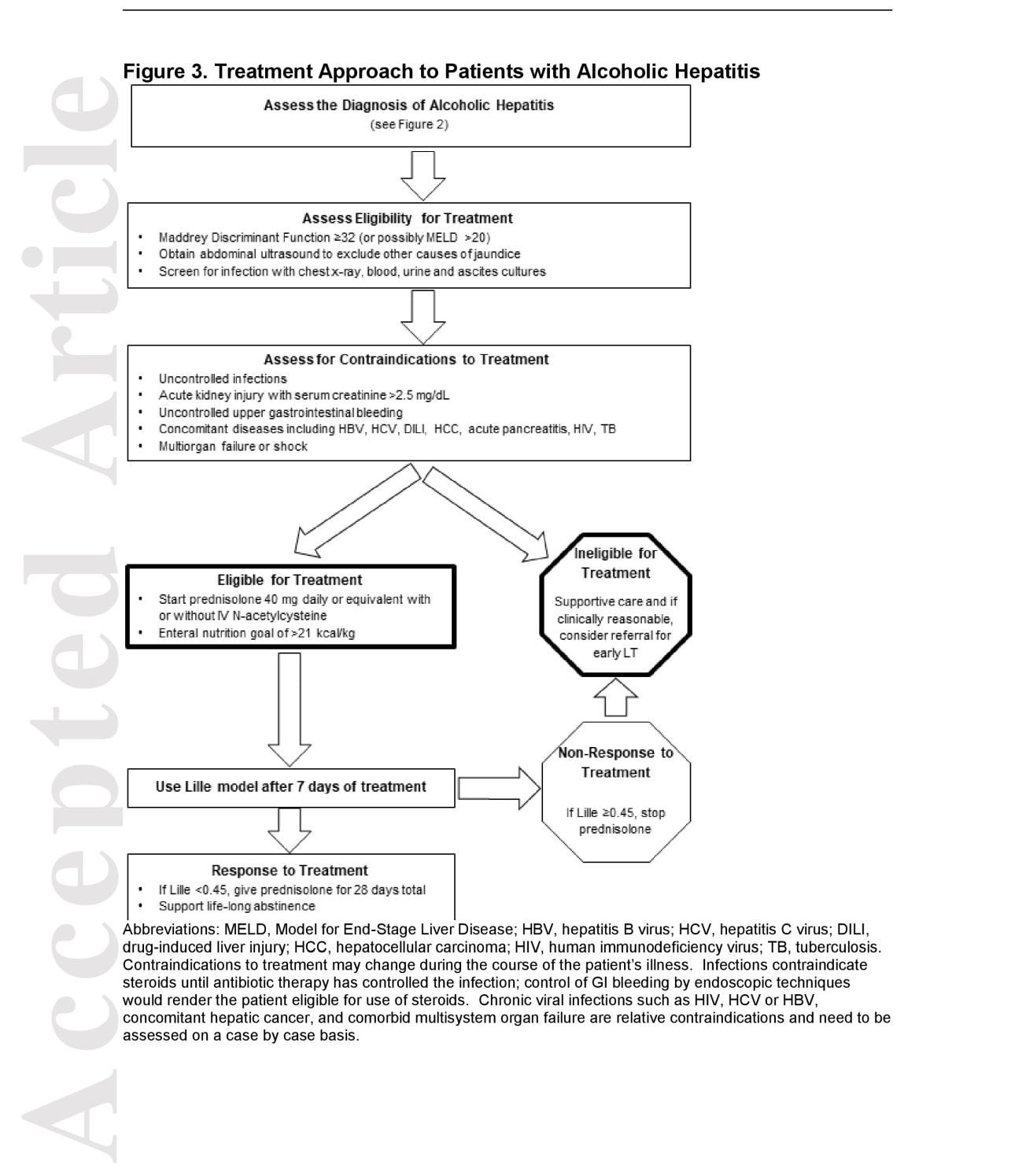
Several validated, lab -based scoring systems can be used to assess the severity and short -term prognosis of AH (Table s 6 and 7). Common elements are shared between the scores, particularly those of the MELD score, and are easily obtained. [129] Providers can use smartphone applications or online calculators like www.lillemodel.com to calculate these scores with careful awareness of the units of measurement being used. These scoring systems perform similarly well in predicting short -term outcome (up to 6 months) in AH. The Maddrey Discriminant Function (MDF) was derived from the results of an early clinical trial comparing corticosteroids to placebo and later modified to identify AH patients with high risk of short-term mortality (30-50% at 28-days) when MDF ≥32. [130] (Figure 3) In contrast, MDF <32 accurately identifies those with mild/moderate AH, conferring low, but not zero, risk of mortality with supportive care. The additional ability to discriminate between patients achieving a survival benefit from corticosteroids and those who do not, has given the MDF time-tested value in patient care and as a universal inclusion criterion in clinical trials of AH. While not validated outside the UK, the Glasgow Alcoholic Hepatitis Score (GAHS) has been shown to further refine the identification of patients with MDF ≥32 who will benefit from corticosteroids (GAHS ≥9), thereby potentially reducing the number needed to treat. [131]
While the MDF is predictive at 1 month, it is less accurate in the intermediate and long-term. The MELD score and the more recently validated Age, serum Bilirubin, INR, and serum Creatinine (ABIC) score provide more nuanced survival prediction by emphasizing impaired renal function and can be calculated at different time points.[132, 133] When there is renal failure but recovering liver function, these scores may give a falsely poor prognosis. While not assessed specifically in patients with severe AH, among patients on the liver transplant waiting list, the ΔMELD score over time reflects progression of liver disease and conveys important additional prognostic information. [134] An increasing MELD score reflects greater risk of death, whereas a declining MELD score reflects a diminution in risk.
Notably, the threshold for initiating liver -specific treatment like corticosteroids has not been established for ABIC or MELD, although MELD >20 has been proposed. [132] The Lille score differs as a dynamic score by incorporating the change in bilirubin at 7 days after starting corticosteroids to assess early treatment response and the utility of its continuation for 28-days. [135] Nonresponse defined by the Lille score >0.45 predicts poor prognosis, supports cessation of corticosteroids and consideration of clinical trial enrollment or early LT.
Calculating the Lille score after 4 days has also been shown to have similar accuracy, potentially reducing unnecessary exposure to corticosteroids even further, although this approach needs additional validation. [136] Combining static and dynamic models to enhance prediction in AH, Louvet et al. demonstrated that the joint -effect model of MELD plus Lille outperformed other combinations such that for a patient with MELD 21 and Lille 0.45 had a 1.9-fold higher risk of death at 2 months than one with MELD 21 and Lille 0.16 (23.7% vs 12.5%). [137] This strategy of combining models improves prediction by incorporating the early change of disease after an intervention and may aid patient care and the design of future clinical trials.
d) 2. Tissue -based Prognostic Scores
There are 2 contemporary liver tissue-based AH prediction models. The alcoholic hepatitis histologic score (AHHS) was derived and validated in a multicenter, international cohort that includes 4 histologic parameters: degree of fibrosis, degree of neutrophil infiltration, type of bilirubinostasis, and presence of megamitochondria. [138] While the AHHS predicted low, moderate and high risk of 90-day mortality with an area under the receiver operating curve (AUR OC) of 0.77, there are concerns about the requirement of liver biopsy (within 48 hours) and significant inter-observer variability among pathologists, limiting its utility. [139] In a proof-of-principle study to incorporate baseline gene expression variables in liver tissue with clinical variables, Trepo et al. devised the gene -signature plus MELD (gs – MELD) scoring system. [140] Combining the expression patterns of 123 genes with the MELD score discriminated patients with poor and good 90 -day survival with an AUROC 0.86 and outperformed other models including MELD plus Lille. While this new score was implemented in an FDA -approved assay platform, it is not yet commercially available for use; further, with liver biopsy done on only a minority of patients with AH, such scores are unlikely to impact practice substantially.
d3) Acute kidney injury in AH
The hemodynamic consequences of portal hypertension that overlap with Systemic Inflammatory Response Syndrome (SIRS) also place patients with AH at high risk for acute kidney injury (AKI) due to hepatorenal syndrome (HRS). [141, 142] The prognostic significance of AKI is reflected in the inclusion of serum creatinine or urea in the AH prognostic scores in Table 6. Strategies to preserve renal function in AH include the avoidance of nephrotoxins like intravenous contrast, aminoglycosides, and non-steroidal anti-inflammatory drugs, and the cautious use of diuretics. Careful surveillance of AKI allows for early treatment with intravenous albumin and vasoconstrictors. [143] Since SIRS is strongly associated with infection, development of multi-organ failure and high mortality in AH, multidisciplinary care involving specialists in hepatology, critical care, infectious disease, nephrology should be provided. [144]
d) 4. Other Prognostic Factors in Alcoholic Hepatitis
The prognostic scores in AH were largely derived and validated in well -defined cohorts receiving corticosteroids. Since a significant proportion of patients with severe AH are ineligible for corticosteroids, these scores may not capture other factors contributing to the protean presentations of severe A H. Infections are common in severe AH with 12 -26% prevalence at the time of admission, with up to half infected at some point while receiving corticosteroids. [145] Infection -related biomarkers like pretreatment serum lipopolysaccharide, bacterial DNA, high -sensitivity C -reactive protein and procalcitonin are associated with the risk of infection and 90-day mortality. [146] Furthermore, as mentioned previously, the presence of systemic inflammatory response syndrome (SIRS) at admission, with or without infection, predicts multiorgan failure (especially AKI) and early death. [147, 148] While the recovery of liver function in short -term prognosis is paramount and captured by the previously discussed prognostic models, in the long-term, abstinence from alcohol is the main driver of outcome in severe AH patients surviving beyond 6 months. [149, 150, 151] Improvement in long-term survival after severe AH should include secondary prevention strategies to promote complete alcohol abstinence.
d) 5. Moderate Alcoholic Hepatitis
To date, little attention has been given to the diagnosis, management, and treatment of patients with AH not meeting the above criteria for severe AH. Such patients might be classified as having moderate AH (which would be define d as having a MELD <20 or MDF >< 32). While there is no well -established therapy for these patients, medical attention should focus on the diagnosis of disease, patient education, referral and interdisciplinary management of these patients with AUD treatment specialists to achieve alcohol cessation. Given the fact that many patients with chronic alcohol use present to medical providers only at the late stage of cirrhosis, early detection of “subclinical” ALD and prevention of progression to AC should be a management goal in both primary care setting as well as in hepatology referrals. Future studies are needed to explore the natural history of moderate AH with regard to its evolution to severe AH and its relationship to the development of cirrhosis in the absence of severe AH.
Guidance Statements
Lab-based prognostic scores should be used to determine prognosis in alcoholic hepatitis.
The Maddrey Discriminant Function ( ≥32) should be used to assess the need for treatment with corticosteroids or other medical therapies.
A MELD score >20 also should prompt consideration of steroid treatment.
Abstinence from alcohol should be promoted to improve long -term prognosis in AH.
e) TREATMENT OF ALCOHOLIC HEPATITIS
e) 1 Treatments of proven benefit
Abstinence
Continued alcohol use in the setting of AH results in increased rates of variceal bleeding, ascites, hepatic encephalopathy, and risk of developing HCC and death. [151, 152, 153, 154] All patients with ALD should be advised to abstain completely from alcohol use, although harm reduction models, which favor alcohol reduction over total abstinence based on a patient’s stated goals, may be appropriate in some contexts.
e) 2 Treatments of likely benefit
Nutritional therapy Nutritional therapy has been studied for decades, as patients with AH are typically very malnourished. [155] Enteral nutritional supplements are recommended by consensus. [156] Two meta -analyses of nutritional support for AH suggested improvement in hepatic encephalopathy and fewer infections, but called for higher quality trials. [157, 158] A recent trial comparing intensive enteral nutrition to conventional nutrition (both arms received corticosteroids ) showed no additional survival benefit of intensive nutrition, with poor toleration of nasogastric tubes and adverse events. [159] Daily calorie intake <21.5 kcal/kg/day was associated with increased rates of infection and mortality at 6-months than those with higher intake (65.8% vs 33.1%; P ><.0001).
Supplementation with specific nutrients has focused on those potentially countering the oxidative stress associated with A H (e.g., beta-carotene, vitamins A, C, and E, and selenium). A meta-analysis found no evidence for benefit in these studies and a comparison of nutritional antioxidants to corticosteroids showed worse outcomes in the antioxidant group. [160, 161] However, most patients with chronic alcohol abuse and AH are zinc deficient. Zinc has been shown to contribute to improving gut mucosal barrier integrity in animal models of ALD and in small pilot human clinical trials. Because of the established role of gut – derived pathogen -associated danger molecules in AH, use of therapeutic doses of zinc should be considered in moderate and severe AH. In AC, recent trials of enteral nutrition have not shown benefit. [160, 162]
Corticosteroids
Corticosteroids are the most extensively studied intervention in AH, with more than 20 clinical trials, including a dozen placebo -controlled trials, dating back more than 40 years. These trials have yielded inconsistent results, with most having a high risk of bias due to heterogeneity and lack of power to detect differences in survival. [163] Further complicating the interpretation of studies and the design of future trials is the declining mortality of severe AH over time, ranging from 30-50% at 28-days in early trials compared to 14 -18% more recently, while several meta -analyses have yielded conflicting conclusions. [130, 151, 164, 165, 166] Mathurin et al. combined the individual patient data sets of three, five, then recently 11 randomized, controlled trials (RCTs), which ultimately included 2111 patients. In the latest iteration, corticosteroid treatment significantly reduced mortality at 28 -days compared to placebo, (hazard rati o, 0.64; 95% CI, 0.48 -0.86) representing a 36% risk reduction. [167, 168, 169]
The largest randomized controlled trial in severe AH is the Steroids or Pentoxifylline for Alcoholic Hepatitis (STOPAH) trial, a multicenter, double -blind, 2 -by -2 factorial, randomized trial, that enrolled 1103 patients with clinically -diagnosed severe AH in the UK over 3 years. [151] The study did not demonstrate a statistically significant survival benefit at 28 -days in patients receiving corticosteroids compared to placebo (odds ratio [OR] 0.72; 95% CI 0.52 –1.01, p= 0.06), whereas, on a post hoc multivariable analysis, corticosteroids were associated with improved 28 -day survival (OR 0.609; p =0.015), but not at 90-days (OR 1.02) or one -year (OR 1.01). The absence of liver biopsy confirmation of diagnosis and lower than expected mortality in the placebo groups may have reduced the ability of the study to identify a positive effect of corticosteroids (assuming one exists). The inclusion of patients with AKI up to serum creatinine 5.7 mg/dL and permitted use of terlipressin may have impacted the benefit of pentoxifylline. The post hoc analysis, which accounted for potential confounders, did demonstrate a short -term survival benefit. The STOPAH trial, taken together with the previously mentioned meta -analys e s, offers modest support for prednisone but not for using pentoxifylline. [170] (Figure 3)
In contrast, a commonly cited Veterans Affairs study in AH patients with MDF >54 receiving corticosteroids were found to have lower survival compared to placebo, suggesting a ceiling beyond which corticosteroids are harmful. [171] However, this study was not powered to examine survival differences at this higher MDF threshold, and subsequent studies have not substantiated this observation. The meta -analysis using individual patient data from 11 RCTs demonstrated that AH patients in the highest MDF quartile (≥68) had statistically similar responses to corticosteroid treatment compared to those with lower MDF scores. [170] This suggests that even very sick patients based on MDF, in the absence of contraindications, can benefit from corticosteroid treatment. Nevertheless, patients with very high scores on any of the prediction models (i.e. MDF >90 or MELD >30) have very severe disease, which necessitates careful assessment for occult infection and other contraindications to corticosteroid treatment.
Evaluating for contraindications to corticosteroids
There are several relative contraindications to corticosteroid use in severe AH. (Figure 3) Since infections (spontaneous bacterial peritonitis, pneumonia, cellulitis, and urinary tract infections) are common in AH and with overlapping clinical presentations, providers should obtain corresponding cultures and a chest radiograph upon presentation. Abdominal imaging (preferably ultrasound with Doppler) is important to evaluate for other causes of jaundice. Sufficient time should be allowed to assess for the presence of infection or other contraindications to treatment with observation and the return of relevant data. For example, the average time from presentation to starting prednisolone from the Lille group (with biopsy) and the STOPAH trial (without biopsy) was within 6 days of presentation. [145, 151] Whether empiric antibiotics in the absence of confirmed infection improves outcomes in severe AH is unknown and is being evaluated in a clinical trial. [172] If infection is present, appropriate antibiotics should be started immediately. While there have been reports of frequent fungal infections resulting in high mortality, particularly Aspergillus species, in corticosteroid -treated AH patients in France and Belgium, [173, 174] this has not been reported elsewhere in Europe or the US. [175, 176] Despite these concerns, the presence of infection alone has not been shown to be a driver of short -term mortality. [145] Rather, the response to corticosteroids based on the Lille score is significantly associated with improved survival as a result of improved liver function despite the presence of infection.
Acute kidney injury has been an exclusion criterion in most AH clinical trials, so the evidence for corticosteroids in patients with AKI is lacking. If AKI can be resolved, corticosteroid treatment should be re-considered. The prognostic significance of AKI in patients with severe AH is discussed in an earlier section.
Patients with gastrointestinal bleeding (GIB) have similarly been excluded in many clinical trials in AH. A retrospective study of 105 patients with biopsy-proven AH, 55% presented with GIB and the remainder did not. [177] Both groups were given prednisolone; GIB patients started at a mean of 5 days after the bleeding episode (mostly variceal hemorrhage). GIB patients had a lower incidence of infections likely due to prophylactic antibiotics, but there were no differences in survival at 1-, 3-, and 6-months between the two groups. This study suggests that GIB is not an absolute contraindication for corticosteroids and that after control of GIB, prednisolone can be given safely.
e) 3 Treatments of potential benefit
N-Acetylcysteine
In a randomized controlled trial in France, co -administration of intravenous N – acetylcysteine (NAC) with corticosteroids reduced some early complications (infection, hepatorenal syndrome) compared to corticosteroids alone. [178] Furthermore, the prednisolone plus NAC arm improved 1-month mortality compared with prednisolone plus placebo (8% vs 24%; P=.006), although this benefit was not seen at 3 or 6 months. Because 6 -month mortality was the primary endpoint, the study was considered a negative trial. The dose, duration, and administration route used were the same as those used for the treatment of acetaminophen and early stage non -acetaminophen acute liver failure. [179, 180] A recent network meta -analysis of 22 randomized controlled trials (2621 patients), also supported the addition of NAC providing survival benefit beyond corticosteroids alone (relative risk 0.28 ; 95% credible interval 0.10-0.69). [181] In summary, prednisolone plus NAC should be considered as promising, but requiring further validation.
Granulocyte-colony stimulating factor (G-CSF) and other interventions
Granulocyte-colony stimulating factor (G-CSF) stimulates liver regeneration. [182] A randomized pilot study comparing pentoxifylline plus G-CSF with pentoxifylline alone for 5 days in severe AH demonstrated significant reduction in prognostic scores and mortality at 90 days with the combination therapy. [183] G-CSF is intriguing on the basis of its capacity to promote hepatic regeneration rather than abrogation of inflammation, but it requires more study (including patients outside of Asia) prior to recommending wider clinical use. [184] Small pilot studies of the antioxidant metadoxine and of fecal microbiota transplantation have also been reported to improv e liver function and survival in patients with AH. These observations require verification before they can be recommended for wider use. [185, 186]
e) 4 Treatments of unlikely benefit
Pentoxifylline and other interventions
The use of pentoxifylline in severe AH was supported by a randomized, controlled trial comparing pentoxifylline to placebo demonstrating a decline in-hospital mortality. [187, 188] Subsequent trials have failed to confirm this survival benefit, but have shown a reduction in the development of HRS in AH patients who received pentoxifylline. [151, 189] Two trials from France failed to show a benefit of pentoxifylline either as a rescue agent in prednisolone non -responders or in combination with prednisolone when compared to prednisolone alone. [188, 190] While the network meta -analysis by Singh et al. did find low -level evidence of benefit, the STOPAH trial and the higher quality meta -analysis of individual patient data have failed to demonstrate any benefit of pentoxifylline. [151, 169, 179]
Clinical trials of tumor necrosis factor -α inhibitors, infliximab and etanercept, in patients with severe AH were terminated early due to infection-related mortality in the treatment arm. [191, 192] Extracorporeal cellular therapy (ELAD) was studied in a multinational, prospective trial that did not show survival benefit compared to standard of care. [193] Older trials of various agents, including antioxidants like S -adenosylmethionine and vitamin E, insulin and glucagon, oxandrolone and propylthiouracil, have failed to demonstrate improvement in survival. [194, 195, 196, 197, 198]
e) 5 Future Treatments
The overlapping pathophysiology of ALD with NASH (impaired fatty acid metabolism, apoptosis, inflammation driven by enteric endotoxin) provides the opportunity for future re – purposing of pharmacologic treatments being developed for NASH. In addition, a major initiative from the NIAAA has supported large multi -institutional consortia with the task of identifying new therapeutic targets and performing early -phase clinical studies to develop and test new treatments for AH. [199, 200] These treatments attempt to influence different pathophysiologic mechanisms in AH, including disrupted gut-barrier function leading to bacterial and endotoxin translocation; innate immune system activation in the liver; and hepatocellular apoptosis, necrosis, and injury.
Guidance Statements
- Prednisolone 40mg/day given orally should be considered to improve 28-day mortality in patients with severe AH (MDF ≥32,) without contraindications to the use of corticosteroids. (Figure 3)
- The addition of intravenous NAC to prednisolone 40 mg/day may improve the 30-day survival of patients with severe AH.
- The Lille score should be used to reassess prognosis, identify non -responders and guide treatment course after 7 days of corticosteroids.
- Patients with AH should have malnutrition addressed and treated, preferably with enteral nutrition.
- Abstinence is key to long -term survival; methods discussed above for treatment of alcohol -use disorders should be utilized to increase abstinence.
- Pentoxifylline is no longer recommended in the treatment of AH.
G. LIVER TRANSPLANTATION FOR ALCOHOL-RELATED LIVER DISEASE
a) PREVALENCE OF LT FOR ALD
ALD is now a leading indication for patients undergoing LT in the US, surpassing HCV infection [12, 201, 202] Either alone or in combination with HCV infection, ALD accounted for 20% of all primary LT in the U.S. from 1988 -2009 (>19,000 recipients), a figure unanticipated by prior expert consensus. [203, 204] Furthermore, in the U.S. between 2004 and 2013 the number of new LT waiting list registrants with ALD increased by 45% from 1400 to 2024%. [205]
The true denominator of ALD patients who could potentially benefit from LT is unknown, so whether patients with ALD are under-referred for LT compared to those with other liver diseases cannot be determined. [206, 207] Negative perceptions among the general public and general practitioners that AUD and ALD are due to failures of personal responsibility, concern about the risk of relapse before and after LT, and the perception of rationing of limited organs also likely reduce appropriate referral. [208] Furthermore, the plasticity of ALD, particularly improvement with abstinence, can render LT less beneficial and confound decisions regarding referral. [209] In contrast, the clinical events surrounding decompensated AC, such as gastrointestinal bleeding or SIRS, mimic or overlap acute on chronic liver failure due to recent alcohol use or co-morbid infection. The complexity of management, lack of access to specialty care and high mortality can limit the emergence of suitable LT candidates. [210]
b) TIMING OF REFERRAL AND SELECTION OF CANDIDATES FOR LT FOR ALD
The clinical indicators that inform the managing provider that LT evaluation should be considered are new onset decompensation (ascites, encephalopathy, jaundice, or variceal hemorrhage), an episode of SBP, diagnosis of HCC, or MELD -Na >21. [170, 211] Patients with ALD who fail to improve after 3 months of abstinence, particularly with Child -Pugh C cirrhosis, should be referred and considered for LT. [209] The selection of appropriate ALD patients for LT is unique amongst LT indications, as the patient’s history of addiction to alcohol is of primary importance. Determining the time of last alcohol use and predicting the likelihood of achieving abstinence before and after LT, are best evaluated by an expert in addiction medicine working within the transplant team. [212, 213, 214]
Up until recently, LT centers in the U.S. required ALD patients to be abstinent from alcohol for a minimum of 6 months prior to listing for LT, often called the 6-month “rule ”. [215] In a 1997 consensus conference of the AASLD and American Society of Transplantation, the 6-month “rule” was justified on the grounds that it allowed time to assess liver recovery that in turn might obviate the need for LT. [216] It also has additional value in more stable patients by ascertaining commitment to abstinence through participation in alcohol rehabilitation. Since then, studies have demonstrated that, while duration of abstinence before LT is linked to future abstinence, the 6 -month “rule” alone is an inadequate predictor of drinking after LT. [217] These studies are confounded by methodological flaws, such as failing to distinguish between a slip (brief alcohol use with regained abstinence after self-recognition of harm) and relapse (a sustained alcohol use of ≥4 drinks in a day, or at least one drink ≥4 days in succession). [218] Furthermore, strict adherence to the 6 month “rule” penalizes some patients with recent drinking who are at low risk of relapse, because they are unlikely to survive that duration. [219] The emergence of early LT for severe AH (discussed below) has changed the dynamic regarding the value of a fixed interval of pre -LT abstinence. Thus, the consensus regarding the appropriateness and application of the 6-month “rule ” appears to be diminishing in the US, just has it has done in Europe. [220]
The AASLD practice guideline recommends that potential LT candidates with ALD undergo evaluation by a mental health provider for full psychiatric diagnosis and adequate treatment planning. [221] A number of groups have attempted to codify the pre -LT psychosocial assessment into a prognostic score: the Michigan alcoholism prognostic scale, the High-Risk Alcoholism Relapse (HRAR), the “Alcohol Relapse Risk Assessment” (ARRA), and the Stanford Integrated Psychosocial Assessment for Transplantation (SIPAT). [222, 223, 224, 225, 226] These scores have some common features such as the favorable value of social integration indicators such as a spouse or partner (sometimes called a “rehabilitation relationship”), stable home and work, and insight into AUD, and the negative significance of a history of failed rehabilitation attempts, or pre -existing psychiatric disorders. [224] Regardless of the evaluation measures, a formal psychological evaluation is only able to separate an AUD LT candidate into high risk or lesser risk strata. Taken together with the complexity of AUD, it follows that there is no single measure that reliably predicts alcohol relapse after LT.
c) OUTCOMES OF LT FOR ALD
Liver allograft and recipient survival for ALD are amongst the highest of all indications for LT. [227] Studies which permit the patient to reveal alcohol use without penalty while on the transplant list suggest that up to 25% will drink during evaluation or waiting for LT. [228] After LT, studies using different methodologies including retrospective review of the medical record, prospective protocol interviews or cross -sectional use of biomarkers like hair, serum, or urine EtG and PEth, show that approximately 20-25% of ALD recipients return to drinking in the first 5 years. [229, 230, 231, 232, 233] Since this is a highly selected group of patients, this may reflect the risk of relapse in the lowest risk stratified population. DiMartini et al. have described several patterns of drinking after LT for ALD, including early relapse with restoration of sobriety, early relapse that persists and relapse after many months of sobriety post -LT. [228] Early recognition of the pattern of relapse may inform tailored interventions to restore sobriety. Relapse to harmful drinking, in contrast to minor slips, has damaging consequences for the liver allograft. New onset AH and recurrent fibrosis in the allograft progressing to cirrhosis are well -documented adverse outcomes post -LT. In a French multicenter study of 712 patients transplanted for ALD between 1990 and 2007, severe relapse – defined as mean alcohol consumption of >20g/d in women and >30 g/d in men for a period of at least 6 months – occurred in 18% (n=128) with a median delay between LT and severe relapse of 25 months. [227] In this group, 32% (n=41) of patients developed cirrhosis after a little over 5 years post -LT (range 1.8-13.9 years). Nearly two – thirds of these individuals died, with a median time from diagnosis of cirrhosis to death being 1.1 years (range 0.1-7.6 years). Furthermore, as mentioned earlier, excessive alcohol use is harmful even when ALD had not been the primary indication cited for LT. [234] This highlights the clandestine nature of AUD and how the role of alcohol may be underappreciated in the LT evaluation. In the post -transplant setting, severe AUD relapse leads to liver fibrosis and cirrhosis in as little as 5 years. [227]
Guidance Statements
- Patients with decompensated alcohol -related cirrhosis, Child -Turcotte -Pugh C or MELD -Na ≥21 should be referred and considered for liver transplantation.
- Candidate selection for liver transplantation in alcohol -related cirrhosis should not be solely based on a fixed interval of abstinence.
d). EARLY LT FOR SEVERE AH
Patients with severe AH not responding to medical therapy have a grim prognosis, with mortality rates as high as 70% at 6 months.135 Until recently, adherence to the 6 month abstinence requirement by most LT centers essentially excluded these patients from consideration for LT. [215] Results from retrospective analyses of explant histology and UNOS data demonstrate similar outcomes of survival and relapse in those with histologic or listing diagnosis of AH compared to ALD patients adhering to the 6 month rule. [235, 236] A seminal prospective, multicenter study in France and Belgium demonstrated that LT performed “early”, prior to six months of abstinence, was life -saving in patients with life -threatening liver failure due to AH. [173] Mathurin et al. applied a rigorous selection process to patients with severe AH having nonresponse to corticosteroids requiring the complete consensus of multiple medical team s prior to wait -listing. Comprehensive psychosocial assessments by an addiction specialist were performed to identify those with lower risk of alcohol relapse. Severe AH as the first liver decompensating event was a key inclusion criterion meant to prioritize those previously unaware of their liver disease from alcohol. After about 90% of severe AH patients who had not responded to steroids were excluded for poor psychosocial profiles, 26 underwent early LT with improved 6 -month survival compared to historical controls (77±8% vs 23±8%; P<.001), low impact on available organs and low rates of relapse. The findings of this trial further challenged the notion of the 6 month waiting period as the only AUD-related criterion for LT eligibility. Efforts to confirm these findings have largely come from the US. [237, 238] A multicenter retrospective American study has extended these observations to 147 patients with AH, median MELD score 39, who underwent LT before 6 months of abstinence (median abstinence 55 days) from 2006 through 2017 at 12 US centers. [239] These patients had no prior diagnosis of liver disease or episodes of AH. Cumulative patient survival after LT was 94% at 1 year and 84% at 3 years, with cumulative incidence of sustained alcohol use of 10% at 1 year (95% CI, 6% -18%) and 17% at 3 years (95% CI, 10% -27%) after LT.
There are several issues that require further study in early LT for AH. The most critical is how best to consistently and uniformly select appropriate patients who have excellent post -LT survival and low risk of relapse post -LT. Since existing studies are limited to severe AH patients not responding to or ineligible for medical therapy presenting with their first liver decompensating event (i.e., no prior diagnosis of liver disease or episodes of AH), these should be important considerations in selecting candidates for early LT. Furthermore, among patients who fulfilled these criteria, the previously mentioned multicenter American study group recently derived a predictive model of 4 pre -LT variables that may identify patients at lo w risk for sustained alcohol use post -LT, but which requires validation. [240] These variables were >10 drinks/day at initial presentation (4 points), multiple prior rehabilitation attempts (4 points), prior alcohol-related legal issues (2 points) and prior illicit substance use (1 point), with a composite “SALT” score <5 having a 95% negative predictive value (95% CI: 89% -98%) for sustained alcohol use post -LT. Also, the optimal use and timing of AUD treatment post -LT remain s to be defined. [241] In addition, there are concerns about potentially negative public perception and its effects on organ donation, which together with the other issues outlined above, have limited wider adoption of this emerging indication for LT. [242]
However, survey and UNOS studies suggest a growing interest in early LT for AH in the US, with at least one -quarter of all centers having performed ≥1 (but most ≤5) with representation from every UNOS region, so consultation with those centers could be considered for a minority of appropriate patients with life -threatening AH. [243, 244]
Guidance Statements
- Liver transplantation may be considered in carefully selected patients with favorable psychosocial profiles in severe AH not responding to medical therapy.
Suggestions for Future Research
The following are important areas in the diagnosis and treatment of patients with alcohol-related liver disease for which additional research/data are needed:
1. Studies providing the accurate assessment of the prevalence of ALD, particularly identifying earlier, asymptomatic stages of ALD such as alcohol -related steatosis or moderate AH, are needed, and may become feasible with broader use of noninvasive steatosis and fibrosis assessment tools.
2. Well-constructed studies of the incidence of alcoholic hepatitis in the US are needed. Particular attention should be paid to diversity of sex, racial background and age.
3. ALD patients have been omitted from studies of efficacy of treatments for AUD. Studies are needed to assess the efficacy of psychosocial and pharmacological treatments in initiating and maintaining abstinence by patients with ALD.
4. The potential for serial measurements of biomarkers in patients with ALD are needed, with the dual endpoints of abstinence and stabilization or improvement in liver disease.
5. Studies of medical agents that abrogate the pathophysiological mechanisms that lead to chronic alcoho -related liver injury are needed. These processes include chronic inflammation, the role of the gut microbiota, progressive fat accumulation, and progressive fibrotic injury.
6. New clinical trials are needed both in moderate (MELD ≤20) and severe AH (MELD > 20) to improve the management of AH.
7. Prospective clinical studies of the utility of liver transplantation (LT) in selected patients with severe AH are needed. In particular, areas for investigation include processes of patient selection, monitoring alcohol use before and after LT and treatment of AUD before and after LT.
Source: https://liverlongevity.com/2019/09/part-1-diagnosis-and-treatment-of-alcohol-related-liver-diseases-2019-practice-guidance-from-the-american-association-for-the-study-of-liver-diseases/