
|
|
|

Newly discovered proteins may protect against aging’s illnesses
November 4, 2018
CON: Patients of Advanced Age Should Not Routinely Undergo Liver Transplantation
September 23, 2019When to Initiate Weight Loss Medications in the NAFLD Population

Authors: Manzhalii Elina, PhD, CEO Global Longevity Institute.
Everyone wants to live an active and healthy life and to live as long as possible. The physicians, scientists, biologists, geneticists, biohackers explore information on the diagnosis of aging, longevity of the indicators on the impact of nutrition, genetics, living conditions, as well as the means of influencing the life expectancy. The scientists around of the the world are looking for drugs for longevity. The developments in science and new technologies inspire confidence in imminent solutions to the problems of radical prolongation of life, and the prevention and treatment of cancer, cirhosis, neurodegenerative diseases, diabet and cardiovascular diseases.
There are potentially massive changes coming to medicine and how we regard aging and treat age-related diseases in the next few decades. With these changes comes the potential for people to live longer and healthier lives thanks to the development of new therapies that directly target the various aging processes in order to delay, prevent, or even reverse age-related diseases. Based on the current pace of technological progress, we assume that therapies that will slow the aging process will be created in the coming years. And in some areas, anti-aging medicine has been successful. Cell products and gene therapies are already here.
The many directions to genetic engineering (GE) humans include:
- a) CAR (chimeric antigen receptors ) T cells already in clinical use;
- b) xenotransplantation currently in preclinical primate trials;
- c) germline (mostly mt (metallothionein)-GE and two autosomal);
- d) hundreds of in vivo and ex vivo gene therapies approved and in development [1].
But there are the following problems. Challenges include testing (long-term) safety and efficacy and bringing down the cost of GE in each of these cases.
Although the geroprotectors discovery is a popular biomedicine trend and more than 200 compounds can slow aging and increase the lifespan of animal models according to the Geroprotectors.org database [2], there are still no geroprotectors on the market. The reasons may be related to the lack of a unified concept of aging mechanisms, the problem of translation of geroprotectors studies results from model organisms to humans, low level of interest from big pharma since aging has no status as a disease [3].
Several pharmacological, dietary, and genetic interventions that increase mammalian lifespan are known, but general principles of lifespan extension remain unclear.
The importance of these treatments cannot be overemphasized, since they will lead to an improvement in the state of health and thus lifespan extension. On the other hand, there is a huge risk for every single one of us that such therapies will appear too late. It would be the greatest tragedy not to live to see the introduction of lifespan-extension therapy, and we are counting years here.
After analyzing scientific articles and stories of long-lived, I found out that there is no universal recipe for longevity as well as the conditions and the events of his past life of these people were significantly different from each other. Super-long-livers and members of their families appear to have certain inherited biological defense factors. If a person is 100, then most likely, one of his parents had lived for a long time, and his children, too, can look forward to a long life. Many of these people have lived more than 110 years old and still a little sore, but often do not lead a healthy lifestyle [4, 40, 41]. Obviously, they have a “protective” gene variants that have contributed to their longevity and resistance to disease.
Moreover, the level of risk of developing age-related diseases such as cancer, cardiovascular disease, dementia, stroke, and also experience a decline in cognitive abilities in groups of centenarians is progressively reduced, indicating that their resistance to these diseases [42]. It is important to identify which genes give it a unique advantage, as well as to understand what and how to control the duration of human life at the genetic level [5, 43]. This is not easy to do. For example a study by sequencing the genome of 17 centenarians aged 110 years or older, found no significant evidence of significant enrichment of the genome of centenarians rare genetic variants of the proteins that would distinguish them from ordinary people [6, 39, 43].
It is known that the life expectancy is influenced by factors such as:
- age over 45 years for men and more than 65 years for women;
- way of life and genetic characteristics;
- ecology and water;
- gastrointestinal health.
Youth and longevity depends on the function of your liver and gut, cardiovascular system and nervous system, endocrine and reproductive systems and of course microbiome.
I especially want to stop on the impact of the gastro – intestinal tract, especially the liver and intestines on life expectancy.
Our youth is directly dependent on the state of the gastrointestinal tract. Because that is where most of the focus of immune protective forces of the body: 80% of the immune system is localized in the intestine. Physiological processes in the intestine contribute to resistance to infectious agents, promote the colonization of the intestinal flora, which synthesizes vitamins as well as a huge number of factors that regulate the growth and differentiation, and also takes part in the regulation of sugar and cholesterol levels.
Any digestive disorders lead to premature aging, the autoimmune mechanism of aging can quickly develop, since the intake of nutrients and antioxidants into the body is disrupted, intestinal permeability is impaired. In turn, the accumulated cellular debris. Hence, skin diseases, cancer and premature aging.
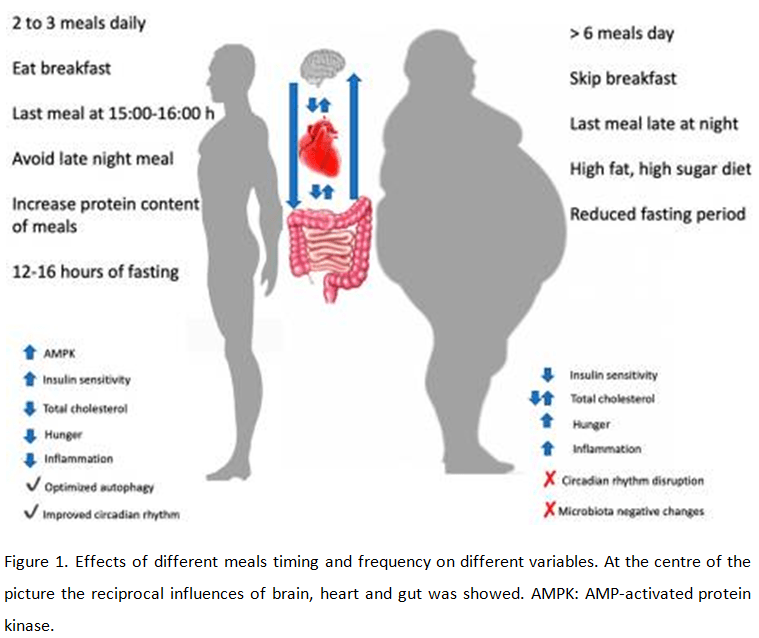
Nutrition affects mutations in genes and can thus change our genome. Nutritional factors can neutralize mutations in genes. Unlike relatively stable genetic information, epigenetic “tags” under certain conditions can be reversible. This fact allows us to rely on a fundamentally new methods of dealing with common diseases, based on eliminating the epigenetic modifications that have emerged in humans under the influence of adverse factors. The use of approaches aimed at correction of the epigenome, opens up great prospects [7, 41, 43]. And in order to fulfill their nutrients function requires the proper functioning of the digestive system, detoxification systems of the liver and intestine. This is the foundation of the basics. (Fig 1.) [8]. We can practically use this data now.
Mankind needs to apply knowledge on how to extend life qualitatively now. People want to be slim, healthy and beautiful right now in real time. And do not wait for the completion of clinical trials in 20 or more years. Our goal is to speed up the process. The solution to the problem is the Global Longevity project.
Global Longevity, just solves the issue of using all the components of longevity already here and now in real time. This unification of all known factors for people who contribute to the maximum longevity. The Project we have focused on the study of the main problems and the common questions that significantly affect life expectancy.
Areas of the Global Longevity Project
- Liver and Longevity. From fatty liver disease to cirrhosis. Ways of solving.
- Brain aging, brain aging rate, prevention of the development of encephalopathy and cerebrovascular diseases.
- Determination of signal biomarkers in the homogenate of the brain and blood.
- Violation of neural connections and the speed of biochemical processes in them.
- The effectiveness of drugs and physical methods in violation of brain function for the prevention of aging.
- The action of pathogenic microorganisms on the aging process of the skin and the correction of skin changes with special bacteria.
In this article we will consider the first direction of an effective solution to the issue of increasing life expectancy. This is liver and longevity. From fatty liver disease to cirrhosis. Ways of solving.
LIVER AND LONGEVITY
As recognition of fatty liver disease and non-alcoholic steatohepatitis (NASH) as a true global health crisis rises the need to curate and emergency treat the disease in a timely fashion grows as well.
The liver is one of the most important organs that affects life expectancy. People who have an unhealthy liver look older by 10-15 years. Liver diseases increase the risk of serious illness. The liver is the largest internal organ in the human body and its proper function is indispensable for many critical metabolic functions, including the regulation of lipid and sugar metabolism, the production of important proteins, including those involved in blood clotting, and purification of blood. The liver is unique in its ability to regenerate in response to injury. A number of evolutionary safeguards have allowed the liver to continue to perform its complex functions despite significant injury. Increased understanding of the regenerative process has significant benefit in the treatment of liver failure. Furthermore, understanding of liver regeneration may shed light on the development of cancer within the cirrhotic liver [9].
There are over 100 described diseases of the liver, and because of its many functions, these can be highly debilitating and life-threatening unless effectively treated. Liver diseases can result from injury to the liver caused by a variety of insults, including hepatitis C virus (HCV), hepatitis B virus (HBV), obesity, chronic excessive alcohol use or autoimmune diseases.
Many people with active liver disease remain undiagnosed largely because liver disease patients are often asymptomatic for many years. According to the European Association for the Study of the Liver (EASL), 29 million Europeans have chronic liver disease, and liver disease represents approximately two percent of deaths annually.
People who have liver disease are 28% more susceptible to viruses and have a greater risk of bacterial infections. Liver diseases lead to a decrease in libido and changes in the condition of the skin and its appendages [10, 11]. Following the epidemic of obesity and type 2 diabetes, non-alcoholic fatty liver disease (NAFLD) is becoming the most frequent liver disease in Western countries. Non-alcoholic steatohepatitis (NASH) is an inflammatory condition caused by fat accumulation in the liver, which presents a serious health concern issue throughout the world, reaching an estimated 5 % prevalence in industrialized countries. It is assumed that NASH originates from a more frequently observed NAFLD characterized by steatosis hepatitis and gamma-glutamyl transferase (GGT) elevation with an estimated prevalence of 25 % in Western and developing countries [12,13,14] .
Established risk factors for disease progression in NAFLD include older age and presence of features of the metabolic syndrome, such as obesity, insulin resistance and hypertension [12]. Genetic factors have also been shown to influence disease progression in NAFLD. Besides the most validated factors influencing lipid metabolism, such as the I148M variant of PNPLA3, the influence of variants involved in fibrogenesis has recently been described [15,16].
Telomeres consist of repeat DNA sequences located at the terminal portion of chromosomes that shorten during mitosis, protecting the tips of chromosomes. During chronic degenerative conditions associated with high cell replication rate, progressive telomere attrition is accentuated, favoring senescence and genomic instability. Several lines of evidence suggest that this process is involved in liver disease progression: (a) telomere shortening and alterations in the expression of proteins protecting the telomere are associated with cirrhosis and hepatocellular carcinoma; (b) advanced liver damage is a feature of a spectrum of genetic diseases impairing telomere function, and inactivating germline mutations in the telomerase complex (including human Telomerase Reverse Transcriptase (hTERT) and human Telomerase RNA Component (hTERC)) are enriched in cirrhotic patients independently of the etiology; and (c) experimental models suggest that telomerase protects from liver fibrosis progression [17].
Genetic data indicate that NAFLD is commonly observed in patients with telomeropathies, suggesting that steatosis may either be a consequence of hepatocellular senescence, as also observed in animal models, or a trigger for liver disease progression [17]. Fibrosis stage and liver disease progression are also strictly linked to cell senescence. Consistently, hepatocyte expression of p21, playing a pivotal role in the induction and maintenance of cellular senescence, was associated with fibrosis stage in NAFLD and increase liver related morbidity and mortality [18]
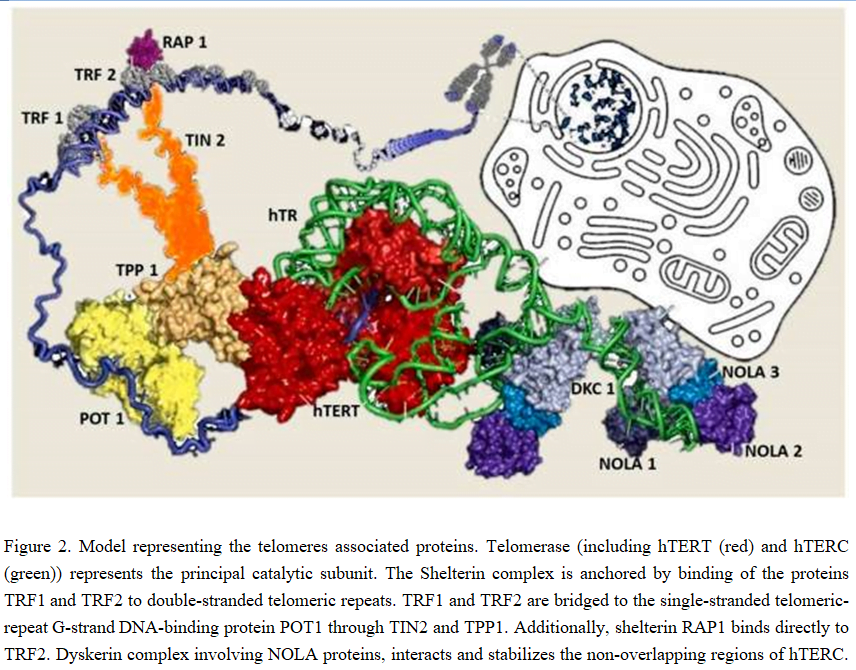
In humans, telomeres consist of thousands copies of six base repeats (TTAGGG) located at the extremities of the chromosomes that protect chromosomes tips from end-to-end fusion, rearrangement and translocation. Telomere length is progressively shortened at each mitosis, due to the inability of the DNA polymerase complex to replicate the very 5′ end of the lagging strand (attrition). For this reason, telomere shortening may function as a “mitotic clock” to sense somatic cells aging. When telomeres become critically short, a DNA-damage program is activated, leading to apoptosis or cell senescence. On the contrary, immortal cells (cancer, stem and germ cells) constitutionally express telomerase, a ribonuclear enzymatic complex associated with telomeres that is responsible for stabilizing telomere length by synthesizing new DNA sequences and adding them to the end of the chromosomes during DNA replication [17]. Telomerase comprises two essential components: Telomerase reverse transcriptase (hTERT) and its RNA template, the telomerase RNA component (hTERC). Dyskerin complex binds to hTERC, in order to protect it and to stabilize the telomerase complex. It includes four nucleolar proteins: Dyskerin (DKC1) and Nucleolar protein family A member 1, 2 and 3 (NOLA1-NOLA2-NOLA3). Besides telomerase, the Shelterin complex, which binds specifically to telomeres, plays a fundamental role in the protection of chromosome ends facilitating telomerase-based telomere elongation. It is composed of six core proteins: the telomeric repeat binding factors 1 and 2 (TRF1-TRF2) that bind telomeric double strand DNA, the protection of telomeres 1 (POT1), which binds the 3′ telomeric region of single strand DNA avoiding the degradation by nuclease, and the TRF-1 interacting protein 2 (TIN2), the POT1-TIN2 organizing protein (TPP1) and the repressor/activator protein 1 (RAP1), that interact with the other proteins bound to telomere stabilizing the complex (Figure 2; [17, 21]). Mutations of proteins involved in maintenance and repair of telomeres are responsible for telomeropathies [19]: a spectrum of progressive genetic diseases exemplified in the most severe cases by dyskeratosis congenita (DKC), whose common autosomal recessive form is caused by mutations in DKC1.
They are degenerative and age-dependent diseases, characterized by premature senescence of the stem cell compartment, determining increased risk of organ failure and cancer, with possible involvement of the hematopoietic compartment, lungs, mucous membranes, skin, and also the liver. Consistently, loss-of-function mutations in hTERT and hTERC may cause a spectrum of familial liver diseases [20]. Telomere length is a strong hereditable tract and telomere shortening is accentuated in chronic degenerative condition associated with high cell replication rate. Thus, involvement of telomeres and telomerase mutations seems to be important in predisposition to liver disease progression towards hepatocellular carcinoma (HCC). Indeed, the incidence of HCC increases with age, and, in particular, in nonalcoholic fatty liver disease (NAFLD), where there is a strong aggregation of familial cases [17,20].
Conversely, reactivation of telomerase occurs during hepatocarcinogenesis, allowing the immortalization of the neoplastic clone. The role of telomere attrition may be particularly relevant in the progression of nonalcoholic fatty liver, an emerging cause of advanced liver disease. Modulation of telomerase or shelterins may be exploited to prevent liver disease progression, and to define specific treatments for different stages of liver disease [17].
The role of ageing in liver fibrosis progression has been largely demonstrated, and older age and duration of liver disease remain the major and more validated risk factors for liver disease progression, together with male gender and alcohol abuse [22, 23, 24].
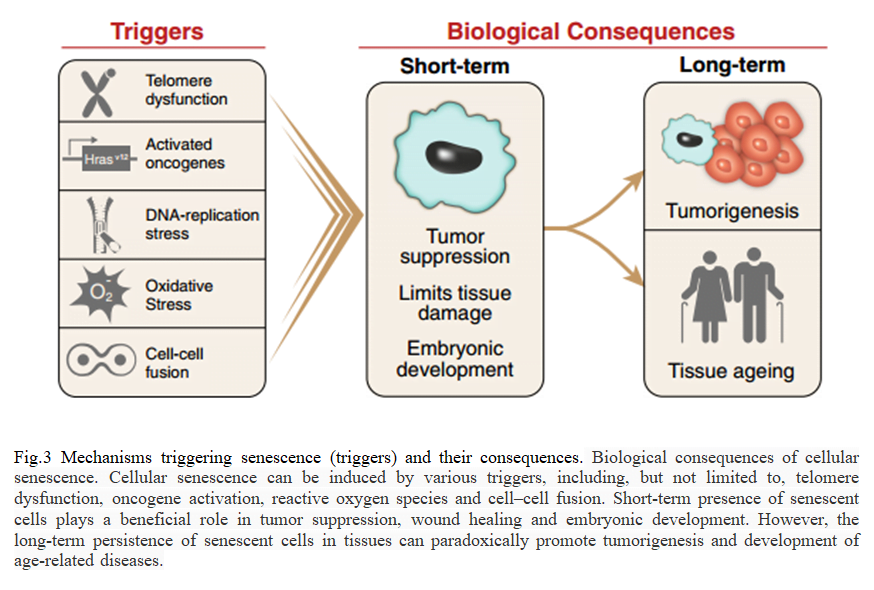
Cellular ageing is generally referred to as replicative senescence, a condition strictly linked to telomerase and telomere biology. Indeed, telomere shortening limited the replicative capacity of cells and the number of cells participating in tissue regeneration. Thus, the regenerative potential of an organ depends on the size of the population of cells with sufficient telomere reserves required for cell proliferation. Consistently, in chronic disease associated with tissue regeneration, such as cirrhosis, an elevated regenerative pressure is generated on the proliferating subpopulation of cells, which undergoes several rounds of cell division that, in turn, accelerate the rate of telomere shortening [17]. When telomeres become critically short, a DNA damage program is activated, leading to cell senescence or apoptosis (due to the Hayflick limit), further reducing the number of cell with regenerative capacity. In response to cellular stress, often resulting in DNA damage, proliferating cells can initiate a program that leads to a permanent cell cycle arrest termed cellular senescence. The short-term induction of cell senescence has beneficial roles in tumor suppression, wound healing and possibly embryonic development (Fig. 3). However, the long-term presence of senescent cells in tissues has the potential to promote age-related disease and cancer in a cell in non-autonomous manner[In response to cellular stress, often resulting in DNA damage, proliferating cells can initiate a program that leads to a permanent cell cycle arrest termed cellular senescence. The short-term induction of cell senescence has beneficial roles in tumor suppression, wound healing and possibly embryonic development (Fig. 3) [25]. However, the long-term presence of senescent cells in tissues has the potential to promote age-related disease and cancer in a cell in non-autonomous manner. In this review, we discuss the various triggers and mechanisms of cell senescence, the physiological and pathological consequences of the senescence program, the ability of senescent cells to interact with immune cells and provide possible explanations for why senescent cells may persist in tissues [25].
Several lines of evidence correlate shortened telomeres with liver fibrosis. Kitada et al. [26] first described a progressive reduction of telomere length during liver disease progression. Urabe et al. [27] confirmed these data and described telomerase re-activation in poorly differentiated HCC, consistently with an increase of telomere length compared to those well differentiated. In the normal liver, progressive telomere shortening has been correlated with age. Consistently, reduction of telomere length in cirrhotic tissue was more marked in patients who developed cirrhosis at younger age [17]. Additionally, reduction of telomere length is considered a hallmark of cirrhotic tissue independently of the etiology of liver disease (e.g., viral hepatitis, autoimmune hepatitis, alcohol abuse…) [28].
Thus, excessive telomere shortening, caused either by telomerase gene mutations or acquired factors, may impair the hepatocyte regenerative ability in response to chronic injury, facilitating fibrosis progression. A causal role of telomere shortening in fibrosis progression has been experimentally demonstrated in telomerase deficient mice. After three generations, these mice developed shortened telomeres and displayed diminished capacity for liver regeneration, and with accelerated development of cirrhosis after liver injury. On the contrary, overexpression of TERT activity improved liver function and protected mice from development of hepatic steatosis and fibrosis [17].
Consistently, shortened telomere length in cirrhotic patients was correlated with the expression of known markers of cellular senescence, such as β-galactosidase, p16, p21 and p53 not only in hepatocytes but also in non-parenchymal cells, such as biliary cells. The p53 protein represents the key regulator point for various signaling pathways of senescence: p53 phosphorylation and consequent activation inhibits cell division primarily inducing p21 expression, which, in turn, activates pRb through inhibition of a cyclin-dependent kinase (Cdk) complex. The activated pRb inhibits the transcription of E2F target genes that are required for cell cycle progression. pRB can alternatively be activated by p16, another Cdk inhibitor, that typically accumulates in senescent cells [17].
Cellular senescence may have a dual role in liver disease: in a first phase, it seems to contribute to liver impairment by reducing the hepatocytes and progenitor cell population, while, in a second phase, the subsequent senescence of HSC (epatic stellate cells) due to long-standing activation of fibrogenesis may protect from further fibrosis progression. In particular, progression of human fibrosis is often characterized by a state of chronic inflammation that results in a condition of cell death and tissue regeneration, involving also a massive expansion of hepatic progenitor cells in order to restore the lost hepatocytes. Ductular reaction typical of this condition has been shown to produce chemotactic stimuli for induction of inflammatory cells and activation of pro-fibrotic hepatic stellate cells (HSC). Moreover, due to the epithelial to mesenchymal transition, progenitors and biliary epithelial cells may provide a portion of myofibroblasts, contributing to fibrosis progression [17]. When the wound is filled, the activated HSC undergo apoptosis or cellular senescence and consequently are eliminated by immune cells. In this way, HSC induce the recruitment of other immune cells at the site of tissue injury that, in turn, help in arresting liver fibrosis progression. However, it has recently been shown that later, senescent HSC may favor HCC development by secreting pro-carcinogenic mediators (the senescence associated secretory program: SASP) [17]. In studies has been shown that in obese people hepatic tissue was characterized by signs of accelerated aging.
Alexander Tyshkovskiy and et. identified hepatic gene signatures associated with lifespan extension across interventions, including upregulation of oxidative phosphorylation and drug metabolism, and showed that perturbed pathways may be shared across tissues. The scientists further applied the discovered longevity signatures to identify new lifespan-extending candidates, such as chronic hypoxia, KU-0063794, and ascorbyl-palmitate [29].
In general, studies show the importance of the role of the liver and gastrointestinal tract in increasing life expectancy. This direction shows the need for further research.
Progression of liver disease to cirrhosis and HCC is generally limited to the subgroup of patients who developed non-alcoholic steatohepatitis (NASH), a condition characterized by active inflammation and fibrosis [13, 23].
Increased inflammation accompanied by the elevation of transaminases (alanine aminotransferase [ALT] > aspartate aminotransferase [AST]) promotes the progression of NASH to fibrosis and, eventually (in > 20 years) to cirrhosis with a potential to develop into hepatocellular carcinoma, which occasionally can occur without cirrhosis . The pathogenesis of NASH is unknown, although the following predisposing factors are considered: obesity, high-calorie/highfat diet, diabetes, hypercholesterolemia, and certain drugs [30]. However, these risk factors may be completely absent, indicating a possible impact of genetic background; thus, mutations in the patatin-like phospholipase domaincontaining-3 (PNPLA3) gene were shown to influence the severity of NAFLD [5]. As NAFLD pathogenesis is not completely understood, effective therapeutic approaches are not yet available. Symptomatic normalization of increased body weight, low-calorie/low fat-diet, lowering of elevated cholesterol levels, optimized therapy for diabetes mellitus, and avoidance of harmful medications are often not completely successful. Nevertheless, these measures should be taken to reduce the risk of hepatic steatosis and inflammation.
There are two main pathways of liver cell death is apoptosis and necrosis.
ALT is an enzyme that is produced in liver cells and is naturally found in the blood of healthy individuals. In liver disease, liver cells are damaged and as a consequence, ALT is released into the blood, increasing ALT levels above the normal range. Physicians routinely test blood levels of ALT to monitor the health of a patient’s liver. ALT level is a clinically important biochemical marker of the severity of liver inflammation and ongoing liver disease.
Elevated levels of ALT represent general markers of liver cell death and inflammation without regard to any specific mechanism. However, in later stage cirrhosis patients, ALT levels have been shown to not be elevated above the normal range. Aspartate aminotransferase (AST) is a second enzyme found in the blood that is produced in the liver and routinely measured by physicians along with ALT. As with ALT, AST is often elevated in liver disease and, like ALT, is considered an overall marker of liver inflammation.
The composition of gastrointestinal microbial community has recently emerged as a new component in the pathogenesis of NASH [31,32]. The conventional view is that bacteria are either destroyed by the gastric acid and phospholipasecontaining pancreatic juice or released with stool. The absorption of bacteria is harmful to the organism and there is no evidence that this process occurs physiologically [7]. Accordingly, only microbial breakdown products or metabolites generated by the intestinal microbiota can have an impact on host metabolism by entering the organism through absorption in the small intestine [11, 31]. Consequently, alterations in the microbial community structure of the gastrointestinal tract may have both potential pathogenic or therapeutic effects on the development of NASH. The treatment options for NASH are currently limited, either because of ineffectiveness as is the case with ursodeoxycholic acid [33], or side effects observed with glitazones or FXR agonists, such as weight gain, arrhythmia, diabetes, or hypercholesterolemia [34]. The impact of adverse events due to drugs may be significant, as the treatment can last for decades, which is necessary because of the natural course of NASH, and may eventually be more damaging than the disease itself. Therefore, it is desirable to develop effective therapeutic approaches without side effects, and the application of natural products may provide a solution to the problem. Probiotics have long been investigated for their health benefits, including those for patients with NASH [35, 36].
In our study, we examined the effect of a cocktail containing Lactobacillus casei, L. rhamnosus, L. bulgaricus, , Bifidobacterium longum, Streptococcus thermophilus and fructooligosaccharides (LBSF) in patients suffering from NASH.
MATERIALS AND METHODS
In this randomized, controlled, non-blinded, prospective clinical trial, 75 patients were diagnosed with NASH. The diagnosis was made based on ultrasonographic detection of steatosis (enhanced echogenicity compared to kidney parenchyma), and elevated serum GGT (> 45 U/L) and ALT (> 40 U/L). Valid transient elastography (fibroscan) test results were also required for participation in the trial. All included patients met these criteria. The exclusion criteria were other chronic liver diseases such as alcoholic steatohepatitis (alcohol consumption of more than 40 g daily for males and more than 20 g daily for females 14), chronic hepatitis B and C, autoimmune hepatitis, Wilson disease, hemochromatosis, and cholestatic liver disease diagnosed based on the anamnesis and standard laboratory procedures. Furthermore, highly obese patients with the body mass index (BMI) > 30, and patients with diabetes (glucose > 100 mg/dL) and hypertriglyceridemia (> 1.7 mmol/L) were also excluded. To avoid patient withdrawal from the trial due to the fear of possible complications caused by liver biopsy as well as for safety reasons, biopsy was not performed in this pilot trial. The enrolled patients were randomly assigned to the experimental group (EG, n = 38) or control group (CG, n = 37).
All NASH patients were provided with basic treatment consisting of a low-fat/low-calorie diet (30–90 g fat/day and 1,800 kcal/day) after appropriate instructions. In addition, the EG patients received LBSF containing Lactobacillus casei, L. rhamnosus, L. bulgaris, Bifidobacterium longum, and Streptococcus thermophilus(108 bacteria/capsule in total) as well as fructooligosaccharides once daily for 12 weeks. Significant suppression of ALT and GGT levels were used as endpoints of the trial, indicating the therapeutic efficacy of LBSF.
Moreover, before and after the 12-week treatment period, all patients underwent a liver ultrasound for evaluation of steatosis and a fibroscan examination (Aixplorer®, Supersonic Imagine, France) with shear wave elastography to obtain objective information about stiffness (elastic properties).
of the liver tissue. In case of a skin capsular distance > 2.5 cm, the obese-specific XL probe was applied. Since in our study highly obese patients were excluded, the XL sensor had only quite rarely been used. Stiffness was determined based on the propagation of elastic waves during 20–30 ultrasonic pulses followed by calculation of the average valid deformation pressure (kPa) with the interquartile range/median value (IQR/M) less than 0.3 15,16. Non-valid measurements with a successful measurement rate < 60 % did not allow the exact determination of liver stiffness and these patients were excluded from the trial. Normal values for healthy livers were 4.1 ± 0.89 kPa (range 2.3–5.9 kPa), and increased stiffness besides fibrosis also indicated in this trial liver inflammation. In addition, glucose, triglycerides, cholesterol, and HDL-cholesterol levels were determined. Microbial composition in stool was quantified by standard techniques [37, 38]. The other parameter considered in the study was adverse events, which included body weight increase or any subjective changes such as heart arrhythmia.
RESULTS
For this trial, we chose patients with NASH, which was defined as steatosis hepatitis with elevated GGT and ALT levels. These patients did not demonstrate clear risk factors for NASH development, but were characterized with the NASH phenotype defined as steatosis hepatitis and elevated GGT and ALT. According to the inclusion criteria, none of the patients had alcoholic steatohepatitis, chronic viral hepatitis (B, C, and D), autoimmune hepatitis, Wilson disease or hemochromatosis, and cholestatic liver disease, as well as treatable or severe metabolic disorders such as obesity, diabetes, and hypertriglyceridemia, which may frequently cause NASH.
Both groups of NASH patients (CG and EG) were instructed to maintain a low calorie/low fat-diet as basic therapy; the EG patients also received the LBSF probiotic cocktail. The demographic characteristics were not different between the groups . Patients in both groups had elevated ALT and GGT levels, and increased BMI and serum cholesterol, as well as higher liver stiffness compared to healthy individuals . In all patients, the low-fat/low-calorie diet resulted in the reduction of the BMI. In the CG patients, a significant decrease of serum cholesterol was detected (P < 0.05), whereas ALT and GGT remained unchanged. In contrast, in EG patients, 12 weeks of therapy with LBSF significantly decreased the levels of ALT and AST (P < 0.05), returning both to the normal range, and improved liver stiffness (P < 0.05). A decrease in GGT was not statistically significant, and steatosis persisted as evidenced by ultrasound examination. Furthermore, the EG patients had a more prominent decrease of the BMI and cholesterol level compared to the CG patients (P < 0.05), while serum glucose and triglyceride remained constantly within the normal range. Analysis of microbial composition in feces revealed in comparison to the standard distribution in healthy subjects (in-house evaluation) that in 50 % of the CG patients the contents of bifidobacteria, lactobacilli, Escherichia coli with normal properties, and Enterococcus faecalis were below normal levels. At the same time, higher concentrations (21–46%) of enterohemorrhagic E. coli, pathogenic enterobacteria, non-pathogenic Staphylococcus, Staphylococcus aureus, Klebsiella, Proteus, Citrobacter, and Candida were detected, which can only be attributed to the low-fat/low-calorie diet.
The application of the probiotic cocktail significantly changed the microbial community structure in the stool of the EG patients. In all cases, an increase towards the normal range was detected, which was not significant only for pathogenic enterobacteria.
The increase of bifidobacteria and lactobacilli in the EG patients was expected, because these microorganisms were constituents of the probiotic cocktail; however, for the other bacterial species the shift to normal levels could be attributed to the indirect beneficial effects of LBSF.
Adverse events were not recorded in any patient during the trial. During the study period, subjective sensations remained unchanged in regard to abdominal discomfort. There were no indications for more frequent urinary infections or heart arrhythmias.
In this short and small-size trial, the efficacy of LBSF for the therapy of NASH was evaluated. The diagnosis of NASH was simplified and based on the following criteria: steatosis and elevation of ALT and GGT. Other chronic liver diseases with obvious etiology, as well as metabolic disorders, including obesity, diabetes, and hypertriglyceridemia were ruled out. The diagnostic criteria applied here describe a subpopulation of NASH patients, which have no other obvious risk factors for NASH development and for whom a potential pathogenic role of gut microbiota could be postulated [30]. Therefore, the rationale for this study was that changes in the bacterial community structure of the gastrointestinal tract with a probiotic cocktail may have a therapeutic effect on NASH patients. If proved successful, such strategy may be potentially beneficial as supportive therapy for metabolic disorders causing NASH. Our results indicate that LBSF, after a short application period of 12 weeks, decreased ALT, and liver stiffness without any adverse events, indicating improvement of the inflammatory status. The change in the microbial composition of the feces was observed after the application of the probiotic cocktail with LBSF, which partially passed through the small intestine to the colon. In the CG, the microbial spectrum showed significant deviations from the normal condition, suggesting that the abnormal bacterial profile in NASH may present a risk for pathogenesis. However, the application of the LBSF cocktail reversed these changes and stabilized the microbial composition in NASH patients, which correlated with the improvement of inflammatory conditions. These data indicate that LBSF intake is clearly beneficial for NASH patients, although the underlying mechanism is unknown. It remains to be determined whether the anti-inflammatory effect such as ALT downregulation can be attributed to metabolic products generated by the re-structured microbial community or the absorption of distinct bacterial fragments, which exert positive effects on the metabolism of NASH patients. The restoration of the microbial structure to the normal state may also be a result of suppression of pathogenic microbes by probiotic bacteria ingested with the cocktail. The strength of the present investigation is the discovery of a potential strategy to improve the inflammatory status in NASH patients by application of a harmless probiotic preparation. It should be noted that in our patients, inflammation, but not steatosis, was decreased. The reduction of liver stiffness may reflect improved tissue elasticity through decreased inflammation rather than resolution of fibrosis, which cannot be expected over the short trial period.
Thus, the anti-inflammatory activity of this probiotic cocktail may not only be applicable to the treatment of NASH, but also to other inflammation-associated liver conditions, including alcoholic steatohepatitis or drug-induced injury. Dietary fat and calorie restriction caused significant weight loss in both patient groups, although the decrease in the BMI was more prominent in the EG compared to CG. The CG patients also had a reduction in total cholesterol levels compared to baseline, which confirms the well-known benefits of low-fat/lowcalorie diet on body weight and cholesterol metabolism. In fact, elevated serum cholesterol was common for our population of NASH patients, and it remains to be determined whether hypercholesterolemia is a causal factor of NASH or just an epiphenomenon. Our pilot study had limitations. First, it was a non-blinded trial based on a small number of patients treated for a short time. Second, patients were diagnosed with NASH based only on GGT and ALT elevation, and detection of steatosis by ultrasonography and enhanced liver stiffness by fibroscan. However, we did not perform biopsy, and, consequently, did not analyze proinflammatory tissue markers. In a confirmatory trial, biopsies at the beginning and end of the study period should be conducted. Third, the trial covered only a small fraction of NASH patients, because those with overt metabolic disorders were excluded. Finally, the mechanism behind the changes of the microbial pattern in NASH patients, and their influence on patient inflammatory state remain to be elucidated.
Nevertheless, this study reveals the strength of this new therapeutic strategy, which should be further evaluated in larger double-blinded randomized controlled trials (RCTs).
Another important marker of liver cell death is a protein fragment called caspase-cleaved Cytokeratin 18 (cCK18). During apoptosis, a key structural protein within the cell called Cytokeratin 18, or CK18, is specifically cleaved by caspases, which results in the release of cCK18 into the blood stream. cCK18 is easily detected in the blood with a commercially-available test and is a mechanism-specific biomarker of apoptosis and caspase activity. Unlike ALT, cCK18 is elevated in patients with advanced liver disease and cirrhosis. Importantly, cCK18 is also present in healthy subjects and multiple studies have demonstrated an approximate basal level in healthy subjects. Numerous independent clinical trials and published studies have demonstrated the utility of cCK18 for detecting and gauging the severity of ongoing liver disease across a variety of disease etiologies. These studies have demonstrated correlations between disease and cCK18 levels in patients with ACLF, LC, portal hypertension (PH), HCV, NASH and various other liver disease indications. For example, it has been shown that in HCV patients, the severity of liver disease was correlated with cCK18 levels and apoptosis, such that the more severe the disease, the higher the serum level of cCK18. In ACLF patients, studies have shown that blood levels of cCK18 were higher in non-surviving patients than in patients that survived. In LC patients, studies have shown that cCK18 levels are elevated and correlate with liver inflammation and cholestasis. cCK18 is a valid and important biomarker of excessive apoptosis in liver disease.
Thus Markers of Liver Cell Death has priority for determining the accelerated aging and should definitely be included in the longevity of the program.
In addition, the first signs of aging appear from the age of 25. So, from this age you need to strengthen measures of control over your body. This means not only body and skin care, balanced nutrition and regular regular exercise, but also prevention and early detection of diseases. Youth and beauty should be both externally and internally.
Therefore, we should measure indicators not only of markers of cell death, but also check up other biomarkers that will signal us about the aging of the body. Medical check up can be an abbreviated or expanded program, which includes a full range of examinations.
Innovative Medical Checkup includes 260 longevity biomarkers such as:
- Complete Blood Cell Count and urine test;
- IGF1 (Somatomedin C) is a marker of the rate of aging and the risk of cancer, dementia and diabetes (once a year, starting at age 21).
- Early signs of cardiovascular disease include high blood pressure, rapid heart rate, and a high level of markers of inflammation in the blood, including the concentration of C-reactive protein (CRP), as well as homocysteine and fibrinogen. Cardiovascular and inflammatory risk: Lipids and inflammation. Apolipoprotrein A1, Apolipoproteine B, Ratio Apo B/ Apo A1. Lipoprotein (А), Cholesterol total, Cholesterol HDL, Cholesterol LOL, Triglycerides, Ultra-sensitive CRP.
- Analyzing hormones. Total Testosterone, Free Testosterone, FSH, LH, Estradiol, Progesteron, Prolactin, Cortizol. Thyroid: TSH, Free T4, Free T3, TG, TPO. Evaluation of imbalance for homocystein, growth hormones, sex hormones, adrenal hormones, pancreatic hormones and thyroid hormone tests. Growth hormones and DHEA-S hormone levels linked to anti-aging, depression, stress and fatigue.
- Uric acid
- Diabetic_risk, insulino-resistance: Fasting glucose, Fasting insulin, HOMA index.
- Marker of DNA damage and oxidative stress of 8-oxo-dGsn. 8-oxo-2′-deoxyguanosine (8-oxo-dG) is an oxidized derivative of deoxyguanosine. 8-oxo-dG is the predominant form of DNA damage from oxidative stress. With age, due to oxidative stress in DNA (a molecule where the genetic code of an organism is encoded), errors and mutations arise. The faster the rate of accumulation of DNA damage and mutations, the faster the aging of the body.
Immune Function Test. Immune system protects you from germs, viruses, and chronic illnesses. Enhance your immune system by testing your NK (Natural Killer) cell activity level. NK cells are “natural killer” cells that respond to and destroy virus-infected cells and tumor cells. Aging is another fundamental factor in the development of cancer. The incidence of cancer increases dramatically with age. This is due to the accumulation of random mutations and epimutations, an age-related decrease in immunity and the effectiveness of DNA repair processes.
- Evaluation of accumulated heavy metals in the body and nutrient mineral imbalances by hair tissue analysis.
- Vitamin B12 and folic acid are mortality and aging brain marker. Folate and vitamin B12 are required both in the methylation of homocysteine to methionine and in the synthesis of S-adenosylmethionine. S-adenosylmethionine is involved in numerous methylation reactions involving proteins, phospholipids, DNA, and neurotransmitter metabolism. Both folate and vitamin B12 deficiency may cause similar neurologic and psychiatric disturbances including depression, dementia, and a demyelinating myelopathy. A current theory proposes that a defect in methylation processes is central to the biochemical basis of the neuropsychiatry of these vitamin deficiencies. Folate deficiency may specifically affect central monoamine metabolism and aggravate depressive disorders. In addition, the neurotoxic effects of homocysteine may also play a role in the neurologic and psychiatric disturbances that are associated with folate and vitamin B12 deficiency.
- Bone health: 25-OH vitamin D, Calcium, Phosphate.
- Iron metabolism: Iron, Ferritin, Transferrin, Soluble receptor TFE
- The glomerular filtration rate is a marker of kidney aging, CVD mortality and prostate cancer risk.
- Human Microbiota. Evaluation of the human body energy metabolism, detoxification function and proliferation of pathogens (bacteria, fungi, helminthic).
- Gastroscopy is the diagnosis of stomach cancer at an early stage.
- Colonoscopy is the diagnosis of colon cancer, as well as the analysis of feces for latent blood is an aybob test (1 every 3 years after 50 years).
- Thickness of the intima-media complex of the common carotid artery.
- Genetic testing provides valuable information about our health that allows us to take the correct measures to improve our health and vitality, as well as prevent potential diseases.
- Physical Measurement and Obesity Index, blood pressure, EKG ;
- Evaluation of functional regulation of the autonomic nervous system by measuring heart rate variability;
The following component of longevity is favorable economic condition of the people.
To live longer with quality of health in modern civilization it is necessary not to ignore medical check their health in childhood. Given the speed of scientific discoveries and the development of new technologies, the state should prioritize anti aging check up programs and allocate funds for them to the budget. This will primarily lead to budget savings, since screening and prevention are cheaper than the cost and ongoing treatment, such as cardio, cancer or obesity. Medical anti aging check up should be accessible to all people in the country. But you must also remember that your quality longevity is first of all necessary for you. Therefore, each family is recommended to lay the family budget is spent on anti aging medical check up.
Social circles that support healthy behaviours are key. A common theme in Longevity is an emphasis on family connection. Children spend time and care for aging parents/grandparents. Committed, long-term relationships with one partner is common. Spending time with children and grandchildren and living close by is also the norm. Working to cultivate your family connection can go a long way.
If you want to live a long healthy life you should surround yourself with like-minded people with positive thinking.
Healthy longevity is impossible without natural ecology.
Natural ecology.
Perfect ecology, fresh air, well- water and widespread gardening provides an opportunity for physical activity, nutritious food and sunlight. This is main factors for longevity.
I observed and studied the centenarians in the mountainous part of Georgia and determined their secret of longevity. The Georgians people have a positive outlook on life and close social support groups. They walk a lot, but they also take time for leisure, and maintain a positive attitude and sense of humor about life. They sleep 8 hours and their diet includes not only nutrient-rich foods like berries, vegetables and greens, but also water that’s naturally high in calcium and magnesium. Every day they use high-quality water with healing properties from mountain sources. In Georgia, more than 730 types of mineral waters are used for balneological purposes and industrial bottling. On the territory of the country more than two thousand sources were discovered, the unique properties of which were known in ancient times and were used to treat various diseases.
Accommodation periodic or stay in such an area uniquely increase the chances of an increase in life expectancy.
In our Global Longevity project, we are just solving this issue.
Global Longevity is the first public project that provides the most comprehensive professional approach to the problem of increasing life expectancy. Global Longevity is a decentralized and scalable ecosystem that creates a full spectrum of living conditions for quality longevity. It uses all the latest achievements of global science and works on the IT platform for the personalized management of life span based on blockchain, neural networks and machine learning. Global Longevity is an ecosystem, a marketplace and a community of users, where technologies will be developed by joint efforts using its own IT platform.
Every person wants to get the whole range of activities available in the world to extend his life, but does not always have full access to full information on this topic.
High technology of longevity.
High technologies of Global Longevity – comprehensive approach to prolonging life.
The mission of Global Longevity is to give people a real opportunity to extend their lives through the use of the advanced longevity technology.
Global Longevity focuses on innovative methods that can be quickly applied to patient health (disease prevention, diagnosis, treatment, diet, physical activity), as well as methods that have long-term goals for life expectancy (new pharmacological, genetic engineering, regenerative, biotechnology). Global Longevity experts examine your personal health, and if they reveal any signs in your body that lead to diseases, they offer a wide range of treatments to make you as healthy as possible. High technology longevity includes the latest new drugs and resources existing in the world to prolong life.
Anti-aging and medical checkup program is aimed at revitalising the entire body and suspension the ageing process. We also recommend high technologies of longevity to people with fatigue, sleep disorder, stress, and hormone syndrome and for prevention of deseases. Depending on the blood results and the anamnesis of the patient, this treatment can be adapted and focused on specific health problem.
Global longevity program includes the definition of biomarkers of longevity.
The Global longevity program includes the following areas:
- Gastroenterology – Longevity:
- Liver longevity
- Gut Longevity
- Comprehensive obesity treatment
- Dietology- Longevity
- Detox – Longevity
- Brain Longevity
- Rejuvanation hair and skin
Longevity program consists of:
- Consultations of the expert of longevity
- Medical checkup
- Psychoanalysis
- Study and restoration of cognitive functions
- Personalized nutrition and lifestyle modifications. Body composition
- Mindtherapy
• Correction and treatment with innovative techniques: geroprotectors such as sirtuins, hormetins, senolytics, quercetin, metformin, sulforaphane, activators of telomerase, glucosamine, biologically active tripeptide GHK (glycyl-L-histidyl-L-lysine), actovegini, resveratrol, lipoic acid, minerals, aminoacids, chelating agents and others. No secondary effects. The rejuvenation program includes only natural products.
Our application of stem cells is used to treat patients in a minimally invasive procedures with maximum results. We use innovative technologies with stem cells as one of the most effective anti-ageing treatment methods.
Stem cells are the basic building blocks of the human body, able to turn into any of 240 types of specialised cells. However, with age, the number of stem cells steadily decreases. That’s one of the reasons for the slower healing of wounds and fractures in the elderly, the higher likelihood of injury and the emergence of a number of chronic diseases. For example, if at birth the content of stem cells in the human body is 1 per 10,000 total cells, then in 50 years there is 1 per 500,000, and at age 70, 1 per 1,000,000. To maintain the body’s regenerative capacity, it’s also possible to bank stem cells.
Stem cells play the crucial role of replacing damaged and ageing cells – something no drug is capable of. When administered to the patient, stem cells migrate to the affected organs and provide restoration of entire biological structures; they also help normalise metabolism, align the body’s immune status and increase resistance to tumours. The programme also has a positive effect on sexual function.
These type of treatments with the advancements that await us in the future, give us the possibility of combating illnesses without the secondary effects that we have nowadays due to pharmaceuticals treatments, as well as the prevention and treatment of many illnesses and conditions including premature aging. If for example we have a damaged liver due to illness and we’re able to transplant the liver with a liver produced by stem cells from the patient (investigation and work that is already in progress), we will be taking a huge step in the direction of a new reality in human longevity and the medical practice.
We all suffer from stress and anxiety from time to time, whether it’s because we are facing a stressful period at work or in our personal life. Whilst sometimes there isn’t much we can do about the circumstances we’re facing, we do have control over how we react to these situations, simply by using the tools that are available to us, like for example, breathing. We forget how important breathing is for our inner balance and wellbeing and by simply doing some breathing exercises throughout the day, we’re able to reduce our cortisol levels and activate our parasympathetic nervous system (PNS) that is responsible for relaxing the body, decreasing heart rate, lowering blood pressure and respiratory rate and diverting blood supply all over the body. Stress management is an important health demand in developed and rapidly developing countries. The principle of stress management consists of four strategies. That is, reduction of stressors, culture of stress tolerance, enrichment of supporting resources, and early detection of manifestations of physical and mental disorders.
Diseases develop and the accumulation of toxins produced mutant defective mitochondria (energy producers in the cell) and reducing their efficiency.
The liver is a major organ of detoxification in the body. It occurs in hepatocytes conversion of xenobiotics (compounds not representing any nutritional value and are potentially toxic) into soluble compounds which are then removed from the body in the bile or in the urine. The process of detoxification in the liver includes two successive stages: phase 1 – oxidation, reduction, hydroxylation and hydrolysis of xenobiotics to intermediate metabolites; Phase 2 – conjugation, methylation, sulfation and glucuronidation of intermediate products to final soluble products. Different xenobiotics, depending on their chemical composition and properties (carcinogens, medicines, drugs) are subjected to various biochemical reactions.
Various methods and agents to increase the life expectancy similarly alter the expression of genes in the liver, although the mechanisms underlying longevity, may also be different.
By understanding what lifestyle habits we should adopt and what nutrition plan suits us best, we can boost our health and prevent premature aging.
Through genetic testing, we can analyse the genetic make-up of each individual and gain a better understanding of our wellness needs. Instead of settling for a generic plan that might work for one person, but not for each individual, you can have access to a fitness plan that is tailored to your DNA, improving the benefits, efficiency and endurance of each individual.
Genetic testing doesn’t only provide valuable information about what the most appropriate workout plan is for each person, but also nutritional advice based on your DNA results. As a result, you’re able to create a personalised nutrition and fitness plan adapted to your needs and provide the best results for your health and wellbeing.
Longevity and health will not be without adequate physical activity.
We are genetically created for movement. Our musculoskeletal system makes up about 80% of body weight. The dependence of life on motor activity is rooted in our genome. The World Health Organization states that physical inactivity is the fourth leading risk factor for death worldwide, and every third person is inactive. Real estate can change the structure and functioning of the brain.
Thus, stress resistance decreases, the risk of developing depression increases, various manifestations of vegetative-vascular dystonia, incomprehensible pains appear that no one can diagnose from the nervous system. On the part of the cardiovascular system, the risk of hypertension and hypotension increases, and the risk of a heart attack doubles. In the genital sphere, a significant reduction of libido and increased risk of gynecological diseases in women and impotence in men increase. Obesity and diabetes develop, and the risk of joint disease increases. People with physical inactivity, are “victims” of constipation is 3 times more than ordinary people. Hemorrhoids are also often associated with these diseases. In addition every fourth case of breast and colon cancer is associated with insufficient physical activity.
Therefore, we need to increase our physical activity in two ways – this is a moderate daily activity and high intensity physical activity. I advise a day of 2-3 hours of moderate physical activity. This can be a quick walk up to 10 thousand steps a day, stairs. This is one of the explanations for the increase in life expectancy in the inhabitants of the mountainous areas of the East. But perform 30 minutes a day of strength training. These are exercises that your doctor will recommend, depending on your health status.
High technologies of longevity programm conduct the systematic analysis on causes of diseases and obesity, including patients’ genetic background, the state of energy metabolism, toxin causing inflammation, and hormone balance. According to the analysis result, a suitable detoxification therapy for blood, intestines, liver, skin is applied to improve the physical constitution and boost energy. In addition, as an individual treatments available simple operation body shape, as well as the outflow of lymph. Our therapies are recommended for those who wish to manage their health in preparation for their middle age or golden years, those who often suffer from minor illness or easily get fatigued, those who want to tone their bodies or get rid of firm fat.
Thus, following the technology developed by Global Longevity, we can now use events to increase life expectancy with the best health and a clear mind and with a beautiful body. This unification and use of all known and available scientific facts that contribute to the maximum quality and longevity longevity (Fig.4).
- The basic rule is to control your life expectancy using the supervision and recommendations of anti-age professionals and experts who will not only prescribe you need examinations for longevity markers, but also correctly evaluate and correct them. Particular attention should be paid to the longevity of the gastrointestinal tract, especially the liver.
- The main economic favorable condition is the availability of all citizens in the country to innovative technologies of longevity.
- To spend more time or purchase housing in ecologically clean areas with access to natural clean products and the possibility of expanding physical activity without vehicles. Minimize stress and overload, use of meditation, respect each other, love people, animals and the environment, constantly improve yourself and learn.
- High longevity biotechnology should be widely applied in practice.
Source: https://liverlongevity.com/